Tuberculosis(TB), also known colloquially as the "white death",or historically asconsumption,[8]is aninfectious diseaseusually caused byMycobacterium tuberculosis(MTB)bacteria.[1]Tuberculosis generally affects thelungs,but it can also affect other parts of the body.[1]Most infections show no symptoms, in which case it is known aslatent tuberculosis.[1]Around 10% of latent infections progress to active disease that, if left untreated, kill about half of those affected.[1]Typical symptoms of active TB are chroniccoughwithblood-containingmucus,fever,night sweats,andweight loss.[1]Infectionof other organs can cause a wide range of symptoms.[9]
| Tuberculosis | |
|---|---|
| Other names | Phthisis, phthisis pulmonalis, consumption, great white plague |
 | |
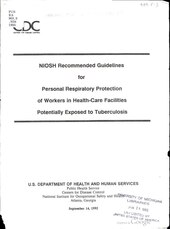
| Chest X-rayof a person with advanced tuberculosis: Infection in both lungs is marked by white arrow-heads, and the formation of a cavity is marked by black arrows. | |
| Specialty | Infectious disease,pulmonology |
| Symptoms | Chronic cough,fever,cough with bloody mucus,weight loss[1] |
| Causes | Mycobacterium tuberculosis[1] |
| Risk factors | Smoking,HIV/AIDS[1] |
| Diagnostic method | CXR,culture,tuberculin skin test,QuantiFERON[1] |
| Differential diagnosis | Pneumonia,histoplasmosis,sarcoidosis,coccidioidomycosis[2] |
| Prevention | Screening those at high risk, treatment of those infected,vaccinationwithbacillus Calmette-Guérin(BCG)[3][4][5] |
| Treatment | Antibiotics[1] |
| Frequency | 25% of people (latent TB)[6] 10.6 million (active TB)[7] |
| Deaths | 1.3 million (2022)[6] |
Tuberculosis isspread from one person to the nextthrough the airwhen people who have active TB in their lungs cough, spit, speak, orsneeze.[1][10]People with latent TB do not spread the disease.[1]Active infection occurs more often in people withHIV/AIDSand in those whosmoke.[1]Diagnosisof active TB is based onchest X-rays,as well asmicroscopicexamination andcultureof bodily fluids.[11]Diagnosis of latent TB relies on thetuberculin skin test(TST) or blood tests.[11]
Prevention of TB involves screening those at high risk, early detection and treatment of cases, andvaccinationwith thebacillus Calmette-Guérin(BCG) vaccine.[3][4][5]Those at high risk include household, workplace, and social contacts of people with active TB.[4]Treatment requires the use of multipleantibioticsover a long period of time.[1]Antibiotic resistanceis a growing problem, with increasing rates ofmultiple drug-resistant tuberculosis(MDR-TB).[1]
In 2018, one quarter of the world's population was thought to have a latent infection of TB.[6]New infections occur in about 1% of the population each year.[12]In 2022, an estimated 10.6 million people developed active TB, resulting in 1.3 million deaths, making it the second leadingcause of death from an infectious diseaseafterCOVID-19.[7]As of 2018, most TB cases occurred in the WHO regions of South-East Asia (44%), Africa (24%), and the Western Pacific (18%), with more than 50% of cases being diagnosed in seven countries: India (27%), China (9%), Indonesia (8%), the Philippines (6%), Pakistan (6%), Nigeria (4%), and Bangladesh (4%).[13]By 2021, the number of new cases each year was decreasing by around 2% annually.[7][1]About 80% of people in many Asian and African countries test positive, while 5–10% of people in the United States test positive via the tuberculin test.[14]Tuberculosis has been present in humans sinceancient times.[15]
History

Tuberculosis has existed sinceantiquity.[15]The oldest unambiguously detectedM. tuberculosisgives evidence of the disease in the remains of bison in Wyoming dated to around 17,000 years ago.[16]However, whether tuberculosis originated in bovines, then transferred to humans, or whether both bovine and human tuberculosis diverged from a common ancestor, remains unclear.[17]A comparison of thegenesofM. tuberculosis complex(MTBC) in humans to MTBC in animals suggests humans did not acquire MTBC from animals during animal domestication, as researchers previously believed. Both strains of the tuberculosis bacteria share a common ancestor, which could have infected humans even before theNeolithic Revolution.[18]Skeletal remains show some prehistoric humans (4000BC) had TB, and researchers have found tubercular decay in the spines ofEgyptianmummiesdating from 3000 to 2400 BC.[19]Genetic studies suggest the presence of TB inthe Americasfrom about AD 100.[20]
Before theIndustrial Revolution,folklore often associated tuberculosis withvampires.When one member of a family died from the disease, the other infected members would lose their health slowly. People believed this was caused by the original person with TB draining the life from the other family members.[21]
Identification
AlthoughRichard Mortonestablished the pulmonary form associated withtuberclesas a pathology in 1689,[22][23]due to the variety of its symptoms, TB was not identified as a single disease until the 1820s.Benjamin Martenconjectured in 1720 that consumptions were caused by microbes which were spread by people living close to each other.[24]In 1819,René Laennecclaimed that tubercles were the cause of pulmonary tuberculosis.[25]J. L. Schönleinfirst published the name "tuberculosis" (German:Tuberkulose) in 1832.[26][27]
Between 1838 and 1845, John Croghan, the owner ofMammoth Cavein Kentucky from 1839 onwards, brought a number of people with tuberculosis into the cave in the hope of curing the disease with the constant temperature and purity of the cave air; each died within a year.[28]Hermann Brehmer opened the first TBsanatoriumin 1859 in Görbersdorf (nowSokołowsko) inSilesia.[29]In 1865,Jean Antoine Villemindemonstrated that tuberculosis could be transmitted, via inoculation, from humans to animals and among animals.[30](Villemin's findings were confirmed in 1867 and 1868 byJohn Burdon-Sanderson.[31])

Robert Kochidentified and described the bacillus causing tuberculosis,M. tuberculosis,on 24 March 1882.[32][33]In 1905, he was awarded theNobel Prize in Physiology or Medicinefor this discovery.[34]
Development of treatments
In Europe, rates of tuberculosis began to rise in the early 1600s to a peak level in the 1800s, when it caused nearly 25% of all deaths.[35]In the 18th and 19th century,tuberculosis had become epidemic in Europe,showing a seasonal pattern.[36][37]Tuberculosis caused widespread public concern in the 19th and early 20th centuries as the disease became common among the urban poor. In 1815, one in four deaths in England was due to "consumption". By 1918, TB still caused one in six deaths in France.[citation needed]
After TB was determined to be contagious, in the 1880s, it was put on anotifiable-diseaselist in Britain. Campaigns started to stop people from spitting in public places, and the infected poor were "encouraged" to entersanatoriathat resembled prisons. The sanatoria for the middle and upper classes offered excellent care and constant medical attention.[29]What later became known as theAlexandra Hospital for Children with Hip Disease(tuberculous arthritis) was opened in London in 1867.[38]Whatever the benefits of the "fresh air" and labor in the sanatoria, even under the best conditions, 50% of those who entered died within five years (c.1916).[29]
Robert Koch did not believe the cattle and human tuberculosis diseases were similar, which delayed the recognition of infected milk as a source of infection. During the first half of the 1900s, the risk of transmission from this source was dramatically reduced after the application of thepasteurizationprocess. Koch announced aglycerineextract of the tubercle bacilli as a "remedy" for tuberculosis in 1890, calling it "tuberculin". Although it was not effective, it was later successfully adapted as a screening test for the presence of pre-symptomatic tuberculosis.[39]World Tuberculosis Dayis marked on 24 March each year, the anniversary of Koch's original scientific announcement. When theMedical Research Councilformed in Britain in 1913, it initially focused on tuberculosis research.[40]
Albert CalmetteandCamille Guérinachieved the first genuine success in immunization against tuberculosis in 1906, using attenuated bovine-strain tuberculosis. It was calledbacille Calmette–Guérin(BCG). The BCG vaccine was first used on humans in 1921 in France,[41]but achieved widespread acceptance in the US, Great Britain, and Germany only after World War II.[42]
By the 1950s mortality in Europe had decreased about 90%.[43]Improvements in sanitation, vaccination, and other public-health measures began significantly reducing rates of tuberculosis even before the arrival ofstreptomycinand other antibiotics, although the disease remained a significant threat.[43]In 1946, the development of the antibiotic streptomycin made effective treatment and cure of TB a reality. Prior to the introduction of this medication, the only treatment was surgical intervention, including the "pneumothoraxtechnique ", which involved collapsing an infected lung to" rest "it and to allow tuberculous lesions to heal.[44]
Current reemergence
Because of the emergence ofmultidrug-resistant tuberculosis(MDR-TB), surgery has been re-introduced for certain cases of TB infections. It involves the removal of infected chest cavities ( "bullae" ) in the lungs to reduce the number of bacteria and to increase exposure of the remaining bacteria to antibiotics in the bloodstream.[45]Hopes of eliminating TB ended with the rise ofdrug-resistantstrains in the 1980s. The subsequent resurgence of tuberculosis resulted in the declaration of a global health emergency by the World Health Organization (WHO) in 1993.[46]
Signs and symptoms

There is a popular misconception that tuberculosis is purely a disease of the lungs that manifests ascoughing.[48]Tuberculosis may infect many organs, even though it most commonly occurs in the lungs (known as pulmonary tuberculosis).[9]Extrapulmonary TB occurs when tuberculosis develops outside of the lungs, although extrapulmonary TB may coexist with pulmonary TB.[9]
General signs and symptoms include fever,chills,night sweats,loss of appetite,weight loss, andfatigue.[9]Significantnail clubbingmay also occur.[49]
Pulmonary
If a tuberculosis infection does become active, it most commonly involves the lungs (in about 90% of cases).[15][50]Symptoms may includechest painand a prolonged cough producing sputum. About 25% of people may not have any symptoms (i.e., they remain asymptomatic).[15]Occasionally, people maycough up bloodin small amounts, and in very rare cases, the infection may erode into thepulmonary arteryor aRasmussen aneurysm,resulting in massive bleeding.[9][51]Tuberculosis may become a chronic illness and cause extensive scarring in the upper lobes of the lungs. The upper lung lobes are more frequently affected by tuberculosis than the lower ones.[9]The reason for this difference is not clear.[14]It may be due to either better air flow,[14]or poorlymphdrainage within the upper lungs.[9]
Extrapulmonary
In 15–20% of active cases, the infection spreads outside the lungs, causing other kinds of TB.[52]These are collectively denoted as extrapulmonary tuberculosis.[53]Extrapulmonary TB occurs more commonly in people with aweakened immune systemand young children. In those with HIV, this occurs in more than 50% of cases.[53]Notable extrapulmonary infection sites include thepleura(in tuberculous pleurisy), thecentral nervous system(intuberculous meningitis), thelymphatic system(inscrofulaof the neck), thegenitourinary system(inurogenital tuberculosis), and thebonesand joints (inPott diseaseof the spine), among others. A potentially more serious, widespread form of TB is called "disseminated tuberculosis"; it is also known asmiliary tuberculosis.[9]Miliary TB currently makes up about 10% of extrapulmonary cases.[54]
Causes
Mycobacteria

The main cause of TB isMycobacterium tuberculosis(MTB), a small,aerobic,nonmotilebacillus.[9]The highlipidcontent of thispathogenaccounts for many of its unique clinical characteristics.[55]Itdividesevery 16 to 20 hours, which is an extremely slow rate compared with other bacteria, which usually divide in less than an hour.[56]Mycobacteria have anouter membranelipid bilayer.[57]If aGram stainis performed, MTB either stains very weakly "Gram-positive" or does not retain dye as a result of the high lipid andmycolic acidcontent of its cell wall.[58]MTB can withstand weakdisinfectantsand survive in adry statefor weeks. In nature, the bacterium can grow only within the cells of ahostorganism, butM. tuberculosiscan be culturedin the laboratory.[59]
Usinghistologicalstains onexpectoratedsamples fromphlegm(also called sputum), scientists can identify MTB under a microscope. Since MTB retains certain stains even after being treated with acidic solution, it is classified as anacid-fast bacillus.[14][58]The most common acid-fast staining techniques are theZiehl–Neelsen stain[60]and theKinyoun stain,which dye acid-fast bacilli a bright red that stands out against a blue background.[61]Auramine-rhodamine staining[62]andfluorescence microscopy[63]are also used.
TheM. tuberculosiscomplex(MTBC) includes four other TB-causingmycobacteria:M. bovis,M. africanum,M. canettii,andM. microti.[64]M. africanumis not widespread, but it is a significant cause of tuberculosis in parts of Africa.[65][66]M. boviswas once a common cause of tuberculosis, but the introduction ofpasteurized milkhas almost eliminated this as a public health problem in developed countries.[14][67]M. canettiiis rare and seems to be limited to theHorn of Africa,although a few cases have been seen in African emigrants.[68][69]M. microtiis also rare and is seen almost only in immunodeficient people, although itsprevalencemay be significantly underestimated.[70]
Other known pathogenic mycobacteria includeM. leprae,M. avium,andM. kansasii.The latter two species are classified as "nontuberculous mycobacteria"(NTM) or atypical mycobacteria. NTM cause neither TB norleprosy,but they do cause lung diseases that resemble TB.[71]

Transmission
When people with active pulmonary TB cough, sneeze, speak, sing, or spit, they expel infectiousaerosoldroplets 0.5 to 5.0μmin diameter. A single sneeze can release up to 40,000 droplets.[72]Each one of these droplets may transmit the disease, since the infectious dose of tuberculosis is very small (the inhalation of fewer than 10 bacteria may cause an infection).[73]
Risk of transmission
People with prolonged, frequent, or close contact with people with TB are at particularly high risk of becoming infected, with an estimated 22% infection rate.[74]A person with active but untreated tuberculosis may infect 10–15 (or more) other people per year.[75]Transmission should occur from only people with active TB – those with latent infection are not thought to be contagious.[14]The probability of transmission from one person to another depends upon several factors, including the number of infectious droplets expelled by the carrier, the effectiveness of ventilation, the duration of exposure, thevirulenceof theM. tuberculosisstrain,the level of immunity in the uninfected person, and others.[76]
The cascade of person-to-person spread can be circumvented by segregating those with active ( "overt" ) TB and putting them on anti-TB drug regimens. After about two weeks of effective treatment, subjects withnonresistantactive infections generally do not remain contagious to others.[74]If someone does become infected, it typically takes three to four weeks before the newly infected person becomes infectious enough to transmit the disease to others.[77]
Risk factors
A number of factors make individuals more susceptible to TB infection and/or disease.[78]
Active disease risk
The most important risk factor globally for developing active TB is concurrent HIV infection; 13% of those with TB are also infected with HIV.[79]This is a particular problem insub-Saharan Africa,where HIV infection rates are high.[80][81]Of those without HIV infection who are infected with tuberculosis, about 5–10% develop active disease during their lifetimes;[49]in contrast, 30% of those co-infected with HIV develop the active disease.[49]
Use of certain medications, such ascorticosteroidsandinfliximab(an anti-αTNF monoclonal antibody), is another important risk factor, especially in thedeveloped world.[15]
Other risk factors include:alcoholism,[15]diabetes mellitus(3-fold increased risk),[82]silicosis(30-fold increased risk),[83]tobacco smoking(2-fold increased risk),[84]indoor air pollution,malnutrition, young age,[78]recently acquired TB infection, recreational drug use, severe kidney disease, low body weight, organ transplant, head and neck cancer,[85]andgenetic susceptibility[86](the overall importance of genetic risk factors remains undefined[15]).
Infection susceptibility
Tobacco smoking increases the risk of infections (in addition to increasing the risk of active disease and death). Additional factors increasing infection susceptibility include young age.[78]
Pathogenesis

About 90% of those infected withM. tuberculosishaveasymptomatic,latent TB infections (sometimes called LTBI),[88]with only a 10% lifetime chance that the latent infection will progress to overt, active tuberculous disease.[89]In those with HIV, the risk of developing active TB increases to nearly 10% a year.[89]If effective treatment is not given, the death rate for active TB cases is up to 66%.[75]

TB infection begins when the mycobacteria reach thealveolar air sacsof the lungs, where they invade and replicate withinendosomesof alveolarmacrophages.[14][90][91]Macrophages identify the bacterium as foreign and attempt to eliminate it byphagocytosis.During this process, the bacterium is enveloped by the macrophage and stored temporarily in a membrane-bound vesicle called a phagosome. The phagosome then combines with a lysosome to create a phagolysosome. In the phagolysosome, the cell attempts to usereactive oxygen speciesand acid to kill the bacterium. However,M. tuberculosishas a thick, waxymycolic acidcapsule that protects it from these toxic substances.M. tuberculosisis able to reproduce inside the macrophage and will eventually kill the immune cell.
The primary site of infection in the lungs, known as theGhon focus,is generally located in either the upper part of the lower lobe, or the lower part of theupper lobe.[14]Tuberculosis of the lungs may also occur via infection from the blood stream. This is known as aSimon focusand is typically found in the top of the lung.[92]This hematogenous transmission can also spread infection to more distant sites, such as peripheral lymph nodes, the kidneys, the brain, and the bones.[14][93]All parts of the body can be affected by the disease, though for unknown reasons it rarely affects theheart,skeletal muscles,pancreas,orthyroid.[94]
Tuberculosis is classified as one of thegranulomatousinflammatory diseases.Macrophages,epithelioid cells,T lymphocytes,B lymphocytes,andfibroblastsaggregate to form granulomas, withlymphocytessurrounding the infected macrophages. When other macrophages attack the infected macrophage, they fuse together to form a giant multinucleated cell in the alveolar lumen. The granuloma may prevent dissemination of the mycobacteria and provide a local environment for interaction of cells of the immune system.[95]
However, more recent evidence suggests that the bacteria use the granulomas to avoid destruction by the host's immune system. Macrophages anddendritic cellsin the granulomas are unable to present antigen to lymphocytes; thus the immune response is suppressed.[96]Bacteria inside the granuloma can become dormant, resulting in latent infection. Another feature of the granulomas is the development of abnormal cell death (necrosis) in the center oftubercles.To the naked eye, this has the texture of soft, white cheese and is termedcaseous necrosis.[95]
If TB bacteria gain entry to the blood stream from an area of damaged tissue, they can spread throughout the body and set up many foci of infection, all appearing as tiny, white tubercles in the tissues.[97]This severe form of TB disease, most common in young children and those with HIV, is called miliary tuberculosis.[98]People with this disseminated TB have a high fatality rate even with treatment (about 30%).[54][99]
In many people, the infection waxes and wanes. Tissue destruction and necrosis are often balanced by healing andfibrosis.[95]Affected tissue is replaced by scarring and cavities filled with caseous necrotic material. During active disease, some of these cavities are joined to the air passages (bronchi) and this material can be coughed up. It contains living bacteria and thus can spread the infection. Treatment with appropriateantibioticskills bacteria and allows healing to take place. Upon cure, affected areas are eventually replaced by scar tissue.[95]
Diagnosis

Active tuberculosis
Diagnosing active tuberculosis based only on signs and symptoms is difficult,[100]as is diagnosing the disease in those who have a weakened immune system.[101]A diagnosis of TB should, however, be considered in those with signs of lung disease orconstitutional symptomslasting longer than two weeks.[101]Achest X-rayand multiplesputum culturesforacid-fast bacilliare typically part of the initial evaluation.[101]Interferon-γ release assays(IGRA) and tuberculin skin tests are of little use in most of the developing world.[102][103]IGRA have similar limitations in those with HIV.[103][104]
A definitive diagnosis of TB is made by identifyingM. tuberculosisin a clinical sample (e.g., sputum,pus,or atissuebiopsy). However, the difficult culture process for this slow-growing organism can take two to six weeks for blood or sputum culture.[105]Thus, treatment is often begun before cultures are confirmed.[106]
Nucleic acid amplification testsandadenosine deaminasetesting may allow rapid diagnosis of TB.[100]Blood tests to detect antibodies are notspecific or sensitive,so they are not recommended.[107]
Latent tuberculosis

TheMantoux tuberculin skin testis often used to screen people at high risk for TB.[101]Those who have been previously immunized with the Bacille Calmette-Guerin vaccine may have a false-positive test result.[108]The test may be falsely negative in those withsarcoidosis,Hodgkin's lymphoma,malnutrition,and most notably, active tuberculosis.[14]Interferon gamma release assays,on a blood sample, are recommended in those who are positive to the Mantoux test.[106]These are not affected by immunization or mostenvironmental mycobacteria,so they generate fewerfalse-positiveresults.[109]However, they are affected byM. szulgai,M. marinum,andM. kansasii.[110]IGRAs may increase sensitivity when used in addition to the skin test, but may be less sensitive than the skin test when used alone.[111]
TheUS Preventive Services Task Force(USPSTF) has recommended screening people who are at high risk for latent tuberculosis with either tuberculin skin tests orinterferon-gamma release assays.[112]While some have recommend testing health care workers, evidence of benefit for this is poor as of 2019[update].[113]TheCenters for Disease Control and Prevention(CDC) stopped recommending yearly testing of health care workers without known exposure in 2019.[114]
Prevention

Tuberculosis prevention and control efforts rely primarily on the vaccination of infants and the detection and appropriate treatment of active cases.[15]TheWorld Health Organization(WHO) has achieved some success with improved treatment regimens, and a small decrease in case numbers.[15]Some countries have legislation to involuntarily detain or examine those suspected to have tuberculosis, orinvoluntarily treatthem if infected.[115]
Vaccines
The only availablevaccineas of 2021[update]isbacillus Calmette-Guérin(BCG).[116][117]In children it decreases the risk of getting the infection by 20% and the risk of infection turning into active disease by nearly 60%.[118][119]
It is the most widely used vaccine worldwide, with more than 90% of all children being vaccinated.[15]The immunity it induces decreases after about ten years.[15]As tuberculosis is uncommon in most of Canada, Western Europe, and the United States, BCG is administered to only those people at high risk.[120][121][122]Part of the reasoning against the use of the vaccine is that it makes the tuberculin skin test falsely positive, reducing the test's usefulness as a screening tool.[122]Several vaccines are being developed.[15]
Intradermal MVA85A vaccine in addition to BCG injection is not effective in preventing tuberculosis.[123]
Public health
Public health campaigns which have focused on overcrowding, public spitting and regular sanitation (including hand washing) during the 1800s helped to either interrupt or slow spread which when combined with contact tracing, isolation and treatment helped to dramatically curb the transmission of both tuberculosis and other airborne diseases which led to theelimination of tuberculosisas a major public health issue in most developed economies.[124][125]Other risk factors which worsened TB spread such as malnutrition were also ameliorated, but since the emergence ofHIVa new population of immunocompromised individuals was available for TB to infect.
Source control in the US
During theHIV/AIDS epidemic in the US,up to 35% of those affected by TB were also infected by HIV.[126]Handling of TB-infected patients in US hospitals was known to create airborne TB that could infect others, especially in unventilated spaces.[127]
Multiple US agencies rolled out new public health rules as a result of the TB spread: theCDCbrought in new guidelines mandatingHEPAfilters andHEPA respirators,[128]NIOSHpushed through new 42 CFR 84 respirator regulations in 1995 (like theN95),[129]andOSHAcreated a proposed rule for TB in 1997, a result of pressure from groups like theLabor Coalition to Fight TB in the Workplace.[130][131]
However, in 2003, OSHA dropped their proposed TB rules, citing a decline of TB in the US, and public disapproval.[132]
Worldwide campaigns
The World Health Organization (WHO) declared TB a "global health emergency" in 1993,[15]and in 2006, the Stop TB Partnership developed aGlobal Plan to Stop Tuberculosisthat aimed to save 14 million lives between its launch and 2015.[133]A number of targets they set were not achieved by 2015, mostly due to the increase in HIV-associated tuberculosis and the emergence of multiple drug-resistant tuberculosis.[15]Atuberculosis classificationsystem developed by theAmerican Thoracic Societyis used primarily in public health programs.[134]In 2015, it launched the End TB Strategy to reduce deaths by 95% and incidence by 90% before 2035. The goal of tuberculosis elimination is being hampered by the lack of rapid testing, short and effective treatment courses, andcompletely effective vaccines.[135]
The benefits and risks of giving anti-tubercular drugs to those exposed to MDR-TB is unclear.[136]Making HAART therapy available to HIV-positive individuals significantly reduces the risk of progression to an active TB infection by up to 90% and can mitigate the spread through this population.[137]
Management

Treatment of TB uses antibiotics to kill the bacteria. Effective TB treatment is difficult, due to the unusual structure and chemical composition of the mycobacterialcell wall,which hinders the entry of drugs and makes many antibiotics ineffective.[138]
Active TB is best treated with combinations of several antibiotics to reduce the risk of the bacteria developingantibiotic resistance.[15]The routine use ofrifabutininstead ofrifampicinin HIV-positive people with tuberculosis is of unclear benefit as of 2007[update].[139]
Acetylsalicylic acid (aspirin) at a dose of 100 mg per day has been shown to improve clinical signs and symptoms, reduce cavitary lesions, lower inflammatory markers, and increase the rate of sputum-negative conversion in patients with pulmonary tuberculosis.[140]
Latent TB
Latent TB is treated with eitherisoniazidorrifampinalone, or a combination of isoniazid with either rifampicin or rifapentine.[141][142][143]
The treatment takes three to nine months depending on the medications used.[76][141][144][143]People with latent infections are treated to prevent them from progressing to active TB disease later in life.[145]
Education or counselling may improve the latent tuberculosis treatment completion rates.[146]
New onset
The recommended treatment of new-onset pulmonary tuberculosis, as of 2010[update],is six months of a combination of antibiotics containing rifampicin, isoniazid,pyrazinamide,andethambutolfor the first two months, and only rifampicin and isoniazid for the last four months.[15]Where resistance to isoniazid is high, ethambutol may be added for the last four months as an alternative.[15]Treatment with anti-TB drugs for at least 6 months results in higher success rates when compared with treatment less than 6 months, even though the difference is small. Shorter treatment regimen may be recommended for those with compliance issues.[147]There is also no evidence to support shorter anti-tuberculosis treatment regimens when compared to a 6-month treatment regimen.[148]However, results presented in 2020 from an international, randomized, controlled clinical trial indicate that a four-month daily treatment regimen containing high-dose, or "optimized", rifapentine with moxifloxacin (2PHZM/2PHM) is as safe and effective as the existing standard six-month daily regimen at curing drug-susceptible tuberculosis (TB) disease.[149]
Recurrent disease
If tuberculosis recurs, testing to determine which antibiotics it is sensitive to is important before determining treatment.[15]Ifmultiple drug-resistant TB(MDR-TB) is detected, treatment with at least four effective antibiotics for 18 to 24 months is recommended.[15]
Medication administration
Directly observed therapy,i.e., having a health care provider watch the person take their medications, is recommended by the World Health Organization (WHO) in an effort to reduce the number of people not appropriately taking antibiotics.[150]The evidence to support this practice over people simply taking their medications independently is of poor quality.[151]There is no strong evidence indicating that directly observed therapy improves the number of people who were cured or the number of people who complete their medicine.[151]Moderate quality evidence suggests that there is also no difference if people are observed at home versus at a clinic, or by a family member versus a health care worker.[151]
Methods to remind people of the importance of treatment and appointments may result in a small but important improvement.[152]There is also not enough evidence to support intermittent rifampicin-containing therapy given two to three times a week has equal effectiveness as daily dose regimen on improving cure rates and reducing relapsing rates.[153]There is also not enough evidence on effectiveness of giving intermittent twice or thrice weekly short course regimen compared to daily dosing regimen in treating children with tuberculosis.[154]
Medication resistance
Primary resistance occurs when a person becomes infected with a resistant strain of TB. A person with fully susceptibleMTBmay develop secondary (acquired) resistance during therapy because of inadequate treatment, not taking the prescribed regimen appropriately (lack of compliance), or using low-quality medication.[155]Drug-resistant TB is a serious public health issue in many developing countries, as its treatment is longer and requires more expensive drugs. MDR-TB is defined as resistance to the two most effective first-line TB drugs: rifampicin and isoniazid. Extensively drug-resistant TB is also resistant to three or more of the six classes of second-line drugs.[156]Totally drug-resistant TB is resistant to all currently used drugs.[157]It was first observed in 2003 in Italy,[158]but not widely reported until 2012,[157][159]and has also been found in Iran and India.[160]There is some efficacy forlinezolidto treat those with XDR-TB but side effects and discontinuation of medications were common.[161][162]Bedaquilineis tentatively supported for use in multiple drug-resistant TB.[163]
XDR-TB is a term sometimes used to defineextensively resistantTB, and constitutes one in ten cases of MDR-TB. Cases of XDR TB have been identified in more than 90% of countries.[160]
For those with known rifampicin or MDR-TB, molecular tests such as the Genotype MTBDRsl Assay (performed on culture isolates or smear positive specimens) may be useful to detect second-line anti-tubercular drug resistance.[164][165]
Prognosis

no data ≤10 10–25 25–50 50–75 75–100 100–250 | 250–500 500–750 750–1000 1000–2000 2000–3000 ≥ 3000 |
Progression from TB infection to overt TB disease occurs when the bacilli overcome the immune system defenses and begin to multiply. In primary TB disease (some 1–5% of cases), this occurs soon after the initial infection.[14]However, in the majority of cases, alatent infectionoccurs with no obvious symptoms.[14]These dormant bacilli produce active tuberculosis in 5–10% of these latent cases, often many years after infection.[49]
The risk of reactivation increases withimmunosuppression,such as that caused by infection with HIV. In people coinfected withM. tuberculosisand HIV, the risk of reactivation increases to 10% per year.[14]Studies usingDNA fingerprintingofM. tuberculosisstrains have shown reinfection contributes more substantially to recurrent TB than previously thought,[167]with estimates that it might account for more than 50% of reactivated cases in areas where TB is common.[168]The chance of death from a case of tuberculosis is about 4% as of 2008[update],down from 8% in 1995.[15]
In people with smear-positive pulmonary TB (without HIV co-infection), after 5 years without treatment, 50–60% die while 20–25% achieve spontaneous resolution (cure). TB is almost always fatal in those with untreated HIV co-infection and death rates are increased even with antiretroviral treatment of HIV.[169]
Epidemiology
Roughly one-quarter of the world's population has been infected withM. tuberculosis,[6]with new infections occurring in about 1% of the population each year.[12]However, most infections withM. tuberculosisdo not cause disease,[170]and 90–95% of infections remain asymptomatic.[88]In 2012, an estimated 8.6 million chronic cases were active.[171]In 2010, 8.8 million new cases of tuberculosis were diagnosed, and 1.20–1.45 million deaths occurred (most of these occurring indeveloping countries).[79][172]Of these, about 0.35 million occur in those also infected with HIV.[173]In 2018, tuberculosis was the leading cause of death worldwide from a single infectious agent.[174]The total number of tuberculosis cases has been decreasing since 2005, while new cases have decreased since 2002.[79]
Tuberculosis[clarification needed]incidence is seasonal, with peaks occurring every spring and summer.[175][176][177][178]The reasons for this are unclear, but may be related to vitamin D deficiency during the winter.[178][179]There are also studies linking tuberculosis to different weather conditions like low temperature, low humidity and low rainfall. It has been suggested that tuberculosis incidence rates may be connected toclimate change.[180]
At-risk groups
Tuberculosis is closely linked to both overcrowding andmalnutrition,making it one of the principaldiseases of poverty.[15]Those at high risk thus include: people who inject illicit drugs, inhabitants and employees of locales where vulnerable people gather (e.g., prisons and homeless shelters), medically underprivileged and resource-poor communities, high-risk ethnic minorities, children in close contact with high-risk category patients, and health-care providers serving these patients.[181]
The rate of tuberculosis varies with age. In Africa, it primarily affects adolescents and young adults.[182]However, in countries where incidence rates have declined dramatically (such as the United States), tuberculosis is mainly a disease of the elderly andimmunocompromised(risk factors are listed above).[14][183]Worldwide, 22 "high-burden" states or countries together experience 80% of cases as well as 83% of deaths.[160]
In Canada and Australia, tuberculosis is many times more common among theIndigenous peoples,especially in remote areas.[184][185]Factors contributing to this include higher prevalence of predisposing health conditions and behaviours, and overcrowding and poverty. In some Canadian Indigenous groups, genetic susceptibility may play a role.[78]
Socioeconomic status (SES) strongly affects TB risk. People of low SES are both more likely to contract TB and to be more severely affected by the disease. Those with low SES are more likely to be affected by risk factors for developing TB (e.g., malnutrition, indoor air pollution, HIV co-infection, etc.), and are additionally more likely to be exposed to crowded and poorly ventilated spaces. Inadequate healthcare also means that people with active disease who facilitate spread are not diagnosed and treated promptly; sick people thus remain in the infectious state and (continue to) spread the infection.[78]
Geographical epidemiology
The distribution of tuberculosis is not uniform across the globe; about 80% of the population in many African, Caribbean, South Asian, and eastern European countries test positive in tuberculin tests, while only 5–10% of the U.S. population test positive.[14]Hopes of totally controlling the disease have been dramatically dampened because of many factors, including the difficulty of developing an effective vaccine, the expensive and time-consuming diagnostic process, the necessity of many months of treatment, the increase in HIV-associated tuberculosis, and the emergence of drug-resistant cases in the 1980s.[15]
In developed countries, tuberculosis is less common and is found mainly in urban areas. In Europe, deaths from TB fell from 500 out of 100,000 in 1850 to 50 out of 100,000 by 1950. Improvements in public health were reducing tuberculosis even before the arrival of antibiotics, although the disease remained a significant threat to public health, such that when theMedical Research Councilwas formed in Britain in 1913 its initial focus was tuberculosis research.[186]
In 2010, rates per 100,000 people in different areas of the world were: globally 178, Africa 332, the Americas 36, Eastern Mediterranean 173, Europe 63, Southeast Asia 278, and Western Pacific 139.[173]
In 2023, tuberculosis overtookCOVID-19as the leading cause of infectious disease-related deaths globally, according to aWorld Health Organization.[187]Around 8.2 million people were newly diagnosed with TB last year, allowing them access to treatment—a record high since WHO’s tracking began in 1995 and an increase from 7.5 million cases in 2022.[188]The report highlights ongoing obstacles in combating TB, including severe funding shortages that hinder efforts toward eradication. Although TB-related deaths decreased slightly to 1.25 million in 2023 from 1.32 million in 2022, the overall number of new cases rose marginally to an estimated 10.8 million.
Russia
Russia has achieved particularly dramatic progress with a decline in its TB mortality rate—from 61.9 per 100,000 in 1965 to 2.7 per 100,000 in 1993;[189][190]however, mortality rate increased to 24 per 100,000 in 2005 and then recoiled to 11 per 100,000 by 2015.[191]
China
China has achieved particularly dramatic progress, with about an 80% reduction in its TB mortality rate between 1990 and 2010.[173]The number of new cases has declined by 17% between 2004 and 2014.[160]
Africa
In 2007, the country with the highest estimated incidence rate of TB wasEswatini,with 1,200 cases per 100,000 people. In 2017, the country with the highest estimatedincidence rateas a % of the population wasLesotho,with 665 cases per 100,000 people.[192]
In South Africa, 54,200 people died in 2022 from TB. The incidence rate was 468 per 100,000 people; in 2015, this was 988 per 100,000. The total incidence was 280,000 in 2022; in 2015, this was 552,000.[193]
India
As of 2017, India had the largest total incidence, with an estimated 2,740,000 cases.[192]According to theWorld Health Organization(WHO), in 2000–2015, India's estimated mortality rate dropped from 55 to 36 per 100,000 population per year with estimated 480 thousand people died of TB in 2015.[194][195]In India a major proportion of tuberculosis patients are being treated by private partners and private hospitals. Evidence indicates that the tuberculosis national survey does not represent the number of cases that are diagnosed and recorded by private clinics and hospitals in India.[196]
North America
In Canada, tuberculosis was endemic in some rural areas as of 1998.[197]The tuberculosis case rate in Canada in 2021 was 4.8 per 100,000 persons. The rates were highest among Inuit (135.1 per 100,000), First Nations (16.1 per 100,000) and people born outside of Canada (12.3 per 100,000).[198]
In the United States,Native Americanshave a fivefold greater mortality from TB,[199]and racial and ethnic minorities accounted for 88% of all reported TB cases.[200]The overall tuberculosis case rate in the United States was 2.9 per 100,000 persons in 2023, representing a 16% increase in cases compared to 2022.[200]
In 2024, Long Beach, California authorized apublic health emergencyin response to a localoutbreakof TB.[201]
Western Europe
In 2017, in the United Kingdom, the national average was 9 per 100,000 and the highest incidence rates inWestern Europewere 20 per 100,000 in Portugal.



Society and culture
Names
Tuberculosis has been known by many names from the technical to the familiar.[204]Phthisis(φθίσις) is the Greek word for consumption, an old term for pulmonary tuberculosis;[8]around 460 BCE,Hippocratesdescribed phthisis as a disease of dry seasons.[205]The abbreviationTBis short fortuberclebacillus.Consumptionwas the most common nineteenth century English word for the disease, and was also in use well into the twentieth century. The Latin rootconmeaning 'completely' is linked tosumeremeaning 'to take up from under'.[206]InThe Life and Death of Mr BadmanbyJohn Bunyan,the author calls consumption "the captain of all these men of death."[207]"Great white plague" has also been used.[204]
Art and literature

Tuberculosis was for centuries associated withpoeticandartisticqualities among those infected, and was also known as "the romantic disease".[204][208]Major artistic figures such as the poetsJohn Keats,Percy Bysshe Shelley,andEdgar Allan Poe,the composerFrédéric Chopin,[209]the playwrightAnton Chekhov,the novelistsFranz Kafka,Katherine Mansfield,[210]Charlotte Brontë,Fyodor Dostoevsky,Thomas Mann,W. Somerset Maugham,[211]George Orwell,[212]andRobert Louis Stevenson,and the artistsAlice Neel,[213]Jean-Antoine Watteau,Elizabeth Siddal,Marie Bashkirtseff,Edvard Munch,Aubrey BeardsleyandAmedeo Modiglianieither had the disease or were surrounded by people who did. A widespread belief was that tuberculosis assisted artistic talent. Physical mechanisms proposed for this effect included the slight fever and toxaemia that it caused, allegedly helping them to see life more clearly and to act decisively.[214][215][216]
Tuberculosis formed an often-reused theme inliterature,as inThomas Mann'sThe Magic Mountain,set in asanatorium;[217]inmusic,as inVan Morrison's song "T.B. Sheets";[218]inopera,as inPuccini'sLa bohèmeandVerdi'sLa Traviata;[216]inart,as inMunch's painting of his ill sister;[219]and infilm,such as the 1945The Bells of St. Mary'sstarringIngrid Bergmanas a nun with tuberculosis.[220]
Public health efforts
In 2014, the WHO adopted the "End TB" strategy which aims to reduce TB incidence by 80% and TB deaths by 90% by 2030.[221]The strategy contains a milestone to reduce TB incidence by 20% and TB deaths by 35% by 2020.[222]However, by 2020 only a 9% reduction in incidence per population was achieved globally, with the European region achieving 19% and the African region achieving 16% reductions.[222]Similarly, the number of deaths only fell by 14%, missing the 2020 milestone of a 35% reduction, with some regions making better progress (31% reduction in Europe and 19% in Africa).[222]Correspondingly, also treatment, prevention and funding milestones were missed in 2020, for example only 6.3 million people were started on TB prevention short of the target of 30 million.[222]
The World Health Organization (WHO), theBill and Melinda Gates Foundation,and the U.S. government are subsidizing a fast-acting diagnostic tuberculosis test for use in low- and middle-income countries as of 2012.[223][224][225]In addition to being fast-acting, the test can determine if there is resistance to the antibiotic rifampicin which may indicate multi-drug resistant tuberculosis and is accurate in those who are also infected with HIV.[223][226]Many resource-poor places as of 2011[update]have access to only sputum microscopy.[227]
India had the highest total number of TB cases worldwide in 2010, in part due to poor disease management within the private and public health care sector.[228]Programs such as theRevised National Tuberculosis Control Programare working to reduce TB levels among people receiving public health care.[229][230]
A 2014EIU-healthcare report finds there is a need to address apathy and urges for increased funding. The report cites among others Lucica Ditui "[TB] is like an orphan. It has been neglected even in countries with a high burden and often forgotten by donors and those investing in health interventions."[160]
Slow progress has led to frustration, expressed by the executive director of theGlobal Fund to Fight AIDS, Tuberculosis and Malaria– Mark Dybul: "we have the tools to end TB as a pandemic and public health threat on the planet, but we are not doing it."[160]Several international organizations are pushing for more transparency in treatment, and more countries are implementing mandatory reporting of cases to the government as of 2014, although adherence is often variable. Commercial treatment providers may at times overprescribe second-line drugs as well as supplementary treatment, promoting demands for further regulations.[160]
The government of Brazil provides universal TB care, which reduces this problem.[160]Conversely, falling rates of TB infection may not relate to the number of programs directed at reducing infection rates but may be tied to an increased level of education, income, and health of the population.[160]Costs of the disease, as calculated by theWorld Bankin 2009 may exceed US$150 billion per year in "high burden" countries.[160]Lack of progress eradicating the disease may also be due to lack of patient follow-up – as among the 250 millionrural migrants in China.[160]
There is insufficient data to show that active contact tracing helps to improve case detection rates for tuberculosis.[231]Interventions such as house-to-house visits, educational leaflets, mass media strategies, educational sessions may increase tuberculosis detection rates in short-term.[232]There is no study that compares new methods of contact tracing such as social network analysis with existing contact tracing methods.[233]
Stigma
Slow progress in preventing the disease may in part be due tostigmaassociated with TB.[160]Stigma may be due to the fear of transmission from affected individuals. This stigma may additionally arise due to links between TB and poverty, and inAfrica, AIDS.[160]Such stigmatization may be both real and perceived; for example, in Ghana, individuals with TB are banned from attending public gatherings.[234]
Stigma towards TB may result in delays in seeking treatment,[160]lower treatment compliance, and family members keeping cause of death secret[234]– allowing the disease to spread further.[160]In contrast, in Russia stigma was associated with increased treatment compliance.[234]TB stigma also affects socially marginalized individuals to a greater degree and varies between regions.[234]
One way to decrease stigma may be through the promotion of "TB clubs", where those infected may share experiences and offer support, or through counseling.[234]Some studies have shown TB education programs to be effective in decreasing stigma, and may thus be effective in increasing treatment adherence.[234]Despite this, studies on the relationship between reduced stigma and mortality are lacking as of 2010[update],and similar efforts to decrease stigma surrounding AIDS have been minimally effective.[234]Some have claimed the stigma to be worse than the disease, and healthcare providers may unintentionally reinforce stigma, as those with TB are often perceived as difficult or otherwise undesirable.[160]A greater understanding of the social and cultural dimensions of tuberculosis may also help with stigma reduction.[235]
Research
The BCG vaccine has limitations and research to develop new TB vaccines is ongoing.[236]A number of potential candidates are currently inphase I and II clinical trials.[236][237]Two main approaches are used to attempt to improve the efficacy of available vaccines. One approach involves adding a subunit vaccine to BCG, while the other strategy is attempting to create new and better live vaccines.[236]MVA85A,an example of a subunit vaccine, is in trials in South Africa as of 2006, is based on a genetically modifiedvacciniavirus.[238]Vaccines are hoped to play a significant role in treatment of both latent and active disease.[239]
To encourage further discovery, researchers and policymakers are promoting new economic models of vaccine development as of 2006, including prizes, tax incentives, andadvance market commitments.[240][241]A number of groups, including theStop TB Partnership,[242]the South African Tuberculosis Vaccine Initiative, and the Aeras Global TB Vaccine Foundation, are involved with research.[243]Among these, the Aeras Global TB Vaccine Foundation received a gift of more than $280 million (US) from theBill and Melinda Gates Foundationto develop and license an improved vaccine against tuberculosis for use in high burden countries.[244][245]
In 2012 a new medication regimen was approved in the US for multidrug-resistant tuberculosis, usingbedaquilineas well as existing drugs. There were initial concerns about the safety of this drug,[246][247][248][249][250]but later research on larger groups found that this regimen improved health outcomes.[251]By 2017 the drug was used in at least 89 countries.[252]Another new drug isdelamanid,which was first approved by the European Medicines Agency in 2013 to be used in multidrug-resistant tuberculosis patients,[253]and by 2017 was used in at least 54 countries.[252]
Steroids add-on therapy has not shown any benefits for active pulmonary tuberculosis infection.[254]
Other animals
Mycobacteria infect many different animals, including birds,[255]fish, rodents,[256]and reptiles.[257]The subspeciesMycobacterium tuberculosis,though, is rarely present in wild animals.[258]An effort to eradicate bovine tuberculosis caused byMycobacterium bovisfrom the cattle and deer herds ofNew Zealandhas been relatively successful.[259]Efforts in Great Britain have been less successful.[260][261]
As of 2015[update],tuberculosis appears to be widespread among captiveelephantsin the US. It is believed that the animals originally acquired the disease from humans, a process calledreverse zoonosis.Because the disease can spread through the air to infect both humans and other animals, it is a public health concern affectingcircusesandzoos.[262][263]
See also
References
- ^abcdefghijklmnop"Tuberculosis (TB)".who.int.Archivedfrom the original on 30 July 2020.Retrieved8 May2020.
- ^Ferri FF (2010).Ferri's differential diagnosis: a practical guide to the differential diagnosis of symptoms, signs, and clinical disorders(2nd ed.). Philadelphia, PA: Elsevier/Mosby. p. Chapter T.ISBN978-0-323-07699-9.
- ^abHawn TR, Day TA, Scriba TJ, Hatherill M, Hanekom WA, Evans TG, et al. (December 2014)."Tuberculosis vaccines and prevention of infection".Microbiology and Molecular Biology Reviews.78(4): 650–71.doi:10.1128/MMBR.00021-14.PMC4248657.PMID25428938.
- ^abcImplementing the WHO Stop TB Strategy: a handbook for national TB control programmes.Geneva:World Health Organization(WHO). 2008. p. 179.ISBN978-92-4-154667-6.Archivedfrom the original on 2 June 2021.Retrieved17 September2017.
- ^abHarris RE (2013)."Epidemiology of Tuberculosis".Epidemiology of chronic disease: global perspectives.Burlington, MA: Jones & Bartlett Learning. p. 682.ISBN978-0-7637-8047-0.Archivedfrom the original on 7 February 2024.Retrieved17 September2017.
- ^abcd"Tuberculosis (TB)".World Health Organization(WHO). 16 February 2018.Archivedfrom the original on 30 December 2013.Retrieved15 September2018.
- ^abc"Tuberculosis (TB)".WHO.Archivedfrom the original on 30 July 2020.Retrieved16 October2021.
- ^abThe Chambers Dictionary.New Delhi: Allied Chambers India Ltd. 1998. p. 352.ISBN978-81-86062-25-8.Archivedfrom the original on 6 September 2015.
- ^abcdefghiAdkinson NF, Bennett JE, Douglas RG, Mandell GL (2010).Mandell, Douglas, and Bennett's principles and practice of infectious diseases(7th ed.). Philadelphia, PA: Churchill Livingstone/Elsevier. p. Chapter 250.ISBN978-0-443-06839-3.
- ^"Basic TB Facts".Centers for Disease Control and Prevention(CDC). 13 March 2012.Archivedfrom the original on 6 February 2016.Retrieved11 February2016.
- ^abKonstantinos A (2010)."Testing for tuberculosis".Australian Prescriber.33(1): 12–18.doi:10.18773/austprescr.2010.005.ISSN0312-8008.
- ^ab"Tuberculosis".World Health Organization (WHO). 2002. Archived fromthe originalon 17 June 2013.
- ^"Global tuberculosis report".World Health Organization (WHO).Archivedfrom the original on 30 December 2013.Retrieved9 November2017.
- ^abcdefghijklmnoKumar V, Robbins SL (2007).Robbins Basic Pathology(8th ed.). Philadelphia: Elsevier.ISBN978-1-4160-2973-1.OCLC69672074.
- ^abcdefghijklmnopqrstuvLawn SD, Zumla AI (July 2011). "Tuberculosis".Lancet.378(9785): 57–72.doi:10.1016/S0140-6736(10)62173-3.PMID21420161.S2CID208791546.
- ^Rothschild BM, Martin LD, Lev G, Bercovier H, Bar-Gal GK, Greenblatt C, et al. (August 2001)."Mycobacterium tuberculosis complex DNA from an extinct bison dated 17,000 years before the present".Clinical Infectious Diseases.33(3): 305–11.doi:10.1086/321886.PMID11438894.
- ^Pearce-Duvet JM (August 2006). "The origin of human pathogens: evaluating the role of agriculture and domestic animals in the evolution of human disease".Biological Reviews of the Cambridge Philosophical Society.81(3): 369–82.doi:10.1017/S1464793106007020.PMID16672105.S2CID6577678.
- ^Comas I, Gagneux S (October 2009). Manchester M (ed.)."The past and future of tuberculosis research".PLOS Pathogens.5(10): e1000600.doi:10.1371/journal.ppat.1000600.PMC2745564.PMID19855821.
- ^Zink AR, Sola C, Reischl U, Grabner W, Rastogi N, Wolf H, et al. (January 2003)."Characterization of Mycobacterium tuberculosis complex DNAs from Egyptian mummies by spoligotyping".Journal of Clinical Microbiology.41(1): 359–67.doi:10.1128/JCM.41.1.359-367.2003.PMC149558.PMID12517873.
- ^Konomi N, Lebwohl E, Mowbray K, Tattersall I, Zhang D (December 2002)."Detection of mycobacterial DNA in Andean mummies".Journal of Clinical Microbiology.40(12): 4738–40.doi:10.1128/JCM.40.12.4738-4740.2002.PMC154635.PMID12454182.
- ^Sledzik PS, Bellantoni N (June 1994)."Brief communication: bioarcheological and biocultural evidence for the New England vampire folk belief"(PDF).American Journal of Physical Anthropology.94(2): 269–74.doi:10.1002/ajpa.1330940210.PMID8085617.Archived(PDF)from the original on 18 February 2017.
- ^Léon Charles Albert CalmetteatWho Named It?
- ^Trail RR (April 1970)."Richard Morton (1637–1698)".Medical History.14(2): 166–74.doi:10.1017/S0025727300015350.PMC1034037.PMID4914685.
- ^Marten B (1720).A New Theory of Consumptions—More Especially a Phthisis or Consumption of the Lungs.London, England: T. Knaplock.Archivedfrom the original on 26 March 2023.Retrieved8 December2020.P. 51: "TheOriginalandEssential Cause... may possibly be some certain Species ofAnimalculaor wonderfully minute living Creatures,... "P. 79:" It may be therefore very likely, that by an habitual lying in the same Bed with a Consumptive Patient, constantly Eating and Drinking with him, or by very frequently conversing so nearly, as to draw in part of the Breath he emits from his Lungs, a Consumption may be caught by a sound Person;... "
- ^Laennec RT (1819).De l'auscultation médiate...(in French). Vol. 1. Paris, France: J.-A. Brosson et J.-S Chaudé. p. 20.Archivedfrom the original on 2 June 2021.Retrieved6 December2020.From p. 20:"L'existence des tubercules dans le poumon est la cause et constitue le charactère anatomique propre de la phthisie pulmonaire (a). (a)... l'effet dont cette maladie tire son nom, c'est-à-dire, la consumption."(The existence of tubercles in the lung is the cause and constitutes the unique anatomical characteristic of pulmonary tuberculosis (a). (a)... the effect from which this malady [pulmonary tuberculosis] takes its name, that is, consumption.)
- ^Schönlein JL (1832).Allgemeine und specielle Pathologie und Therapie[General and Special Pathology and Therapy] (in German). Vol. 3. Würzburg, (Germany): C. Etlinger. p. 103.Archivedfrom the original on 2 June 2021.Retrieved6 December2020.
- ^The word "tuberculosis" first appeared in Schönlein's clinical notes in 1829. See:Jay SJ, Kırbıyık U, Woods JR, Steele GA, Hoyt GR, Schwengber RB, et al. (November 2018). "Modern theory of tuberculosis: culturomic analysis of its historical origin in Europe and North America".The International Journal of Tuberculosis and Lung Disease.22(11): 1249–1257.doi:10.5588/ijtld.18.0239.PMID30355403.S2CID53027676.See especially Appendix, p. iii.
- ^"Kentucky: Mammoth Cave long on history".CNN.27 February 2004. Archived fromthe originalon 13 August 2006.Retrieved8 October2006.
- ^abcMcCarthy OR (August 2001)."The key to the sanatoria".Journal of the Royal Society of Medicine.94(8): 413–17.doi:10.1177/014107680109400813.PMC1281640.PMID11461990.Archivedfrom the original on 3 August 2012.Retrieved28 September2011.
- ^Villemin JA (1865)."Cause et nature de la tuberculose"[Cause and nature of tuberculosis].Bulletin de l'Académie Impériale de Médecine(in French).31:211–216.Archivedfrom the original on 9 December 2021.Retrieved6 December2020.
- See also:Villemin JA (1868).Etudes sur la tuberculose: preuves rationnelles et expérimentales de sa spécificité et de son inoculabilité[Studies of tuberculosis: rational and experimental evidence of its specificity and inoculability] (in French). Paris, France: J.-B. Baillière et fils.Archivedfrom the original on 7 February 2024.Retrieved6 December2020.
- ^Burdon-Sanderson, John Scott. (1870) "Introductory Report on the Intimate Pathology of Contagion." Appendix to: Twelfth Report to the Lords of Her Majesty's Most Honourable Privy Council of the Medical Officer of the Privy Council [for the year 1869], Parliamentary Papers (1870), vol. 38, 229–256.
- ^Koch R (24 March 1882)."Die Ätiologie der Tuberkulose (1882)".Robert Koch: Zentrale Texte[The Etiology of Tuberculosis]. Klassische Texte der Wissenschaft. Vol. 19. Berlin, Heidelberg: Springer Spektrum. pp. 221–30.doi:10.1007/978-3-662-56454-7_4.ISBN978-3-662-56454-7.Archivedfrom the original on 6 November 2018.Retrieved15 June2021.
- ^"History: World TB Day".Centers for Disease Control and Prevention(CDC). 12 December 2016.Archivedfrom the original on 7 December 2018.Retrieved23 March2019.
- ^"The Nobel Prize in Physiology or Medicine 1905".www.nobelprize.org.Archivedfrom the original on 10 December 2006.Retrieved7 October2006.
- ^Bloom BR (1994).Tuberculosis: pathogenesis, protection, and control.Washington, DC: ASM Press.ISBN978-1-55581-072-6.
- ^Frith J."History of Tuberculosis. Part 1 – Phthisis, consumption and the White Plague".Journal of Military and Veterans' Health.Archivedfrom the original on 8 April 2021.Retrieved26 February2021.
- ^Zürcher K, Zwahlen M, Ballif M, Rieder HL, Egger M, Fenner L (5 October 2016)."Influenza Pandemics and Tuberculosis Mortality in 1889 and 1918: Analysis of Historical Data from Switzerland".PLOS ONE.11(10): e0162575.Bibcode:2016PLoSO..1162575Z.doi:10.1371/journal.pone.0162575.PMC5051959.PMID27706149.
- ^"Lost Hospitals of London".ezitis.myzen.co.uk.Retrieved27 June2024.
- ^Waddington K (January 2004)."To stamp out 'so terrible a malady': bovine tuberculosis and tuberculin testing in Britain, 1890–1939".Medical History.48(1): 29–48.doi:10.1017/S0025727300007043.PMC546294.PMID14968644.
- ^Hannaway C (2008).Biomedicine in the twentieth century: practices, policies, and politics.Amsterdam: IOS Press. p. 233.ISBN978-1-58603-832-8.Archivedfrom the original on 7 September 2015.
- ^Bonah C (December 2005). "The 'experimental stable' of the BCG vaccine: safety, efficacy, proof, and standards, 1921–1933".Studies in History and Philosophy of Biological and Biomedical Sciences.36(4): 696–721.doi:10.1016/j.shpsc.2005.09.003.PMID16337557.
- ^Comstock GW (September 1994). "The International Tuberculosis Campaign: a pioneering venture in mass vaccination and research".Clinical Infectious Diseases.19(3): 528–40.doi:10.1093/clinids/19.3.528.PMID7811874.
- ^abPersson S (2010).Smallpox, Syphilis and Salvation: Medical Breakthroughs That Changed the World.ReadHowYouWant.com. p. 141.ISBN978-1-4587-6712-7.Archivedfrom the original on 6 September 2015.
- ^Shields T (2009).General thoracic surgery(7th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 792.ISBN978-0-7817-7982-1.Archivedfrom the original on 6 September 2015.
- ^Lalloo UG, Naidoo R, Ambaram A (May 2006). "Recent advances in the medical and surgical treatment of multi-drug resistant tuberculosis".Current Opinion in Pulmonary Medicine.12(3): 179–85.doi:10.1097/01.mcp.0000219266.27439.52.PMID16582672.S2CID24221563.
- ^"Frequently asked questions about TB and HIV".World Health Organization (WHO). Archived fromthe originalon 8 August 2011.Retrieved15 April2012.
- ^Schiffman G (15 January 2009)."Tuberculosis Symptoms".eMedicine Health.Archivedfrom the original on 16 May 2009.
- ^Kamboj A, Lause M, Kamboj K (2023). "The Problem of Tuberculosis: Myths, Stigma, and Mimics". In Rezaei N (ed.).Tuberculosis.Integrated Science. Vol. 11. Springer. pp. 1046–1062.doi:10.1007/978-3-031-15955-8_50.ISBN978-3-031-15954-1.
- ^abcdGibson PG, Abramson M, Wood-Baker R, Volmink J, Hensley M, Costabel U, eds. (2005).Evidence-Based Respiratory Medicine(1st ed.). BMJ Books. p. 321.ISBN978-0-7279-1605-1.Archivedfrom the original on 8 December 2015.
- ^Behera D (2010).Textbook of Pulmonary Medicine(2nd ed.). New Delhi: Jaypee Brothers Medical Publishers. p. 457.ISBN978-81-8448-749-7.Archivedfrom the original on 6 September 2015.
- ^Halezeroğlu S, Okur E (March 2014)."Thoracic surgery for haemoptysis in the context of tuberculosis: what is the best management approach?".Journal of Thoracic Disease.6(3): 182–85.doi:10.3978/j.issn.2072-1439.2013.12.25.PMC3949181.PMID24624281.
- ^Jindal SK, ed. (2011).Textbook of Pulmonary and Critical Care Medicine.New Delhi: Jaypee Brothers Medical Publishers. p. 549.ISBN978-93-5025-073-0.Archivedfrom the original on 7 September 2015.
- ^abGolden MP, Vikram HR (November 2005). "Extrapulmonary tuberculosis: an overview".American Family Physician.72(9): 1761–68.PMID16300038.
- ^abHabermann TM, Ghosh A (2008).Mayo Clinic internal medicine: concise textbook.Rochester, MN: Mayo Clinic Scientific Press. p. 789.ISBN978-1-4200-6749-1.Archivedfrom the original on 6 September 2015.
- ^Southwick F (2007). "Chapter 4: Pulmonary Infections".Infectious Diseases: A Clinical Short Course, 2nd ed.McGraw-Hill Medical Publishing Division. pp. 104, 313–14.ISBN978-0-07-147722-2.
- ^Jindal SK (2011).Textbook of Pulmonary and Critical Care Medicine.New Delhi: Jaypee Brothers Medical Publishers. p. 525.ISBN978-93-5025-073-0.Archivedfrom the original on 6 September 2015.
- ^Niederweis M, Danilchanka O, Huff J, Hoffmann C, Engelhardt H (March 2010)."Mycobacterial outer membranes: in search of proteins".Trends in Microbiology.18(3): 109–16.doi:10.1016/j.tim.2009.12.005.PMC2931330.PMID20060722.
- ^abMadison BM (May 2001). "Application of stains in clinical microbiology".Biotechnic & Histochemistry.76(3): 119–25.doi:10.1080/714028138.PMID11475314.
- ^Parish T, Stoker NG (December 1999)."Mycobacteria: bugs and bugbears (two steps forward and one step back)".Molecular Biotechnology.13(3): 191–200.doi:10.1385/MB:13:3:191.PMID10934532.S2CID28960959.
- ^Medical Laboratory Science: Theory and Practice.New Delhi: Tata McGraw-Hill. 2000. p. 473.ISBN978-0-07-463223-9.Archivedfrom the original on 6 September 2015.
- ^"Acid-Fast Stain Protocols".21 August 2013. Archived fromthe originalon 1 October 2011.Retrieved26 March2016.
- ^Kommareddi S, Abramowsky CR, Swinehart GL, Hrabak L (November 1984). "Nontuberculous mycobacterial infections: comparison of the fluorescent auramine-O and Ziehl-Neelsen techniques in tissue diagnosis".Human Pathology.15(11): 1085–9.doi:10.1016/S0046-8177(84)80253-1.PMID6208117.
- ^van Lettow M, Whalen C (2008). Semba RD, Bloem MW (eds.).Nutrition and health in developing countries(2nd ed.). Totowa, N.J.: Humana Press. p. 291.ISBN978-1-934115-24-4.Archivedfrom the original on 6 September 2015.
- ^van Soolingen D, Hoogenboezem T, de Haas PE, Hermans PW, Koedam MA, Teppema KS, et al. (October 1997)."A novel pathogenic taxon of the Mycobacterium tuberculosis complex, Canetti: characterization of an exceptional isolate from Africa".International Journal of Systematic Bacteriology.47(4): 1236–45.doi:10.1099/00207713-47-4-1236.PMID9336935.
- ^Niemann S, Rüsch-Gerdes S, Joloba ML, Whalen CC, Guwatudde D, Ellner JJ, et al. (September 2002)."Mycobacterium africanum subtype II is associated with two distinct genotypes and is a major cause of human tuberculosis in Kampala, Uganda".Journal of Clinical Microbiology.40(9): 3398–405.doi:10.1128/JCM.40.9.3398-3405.2002.PMC130701.PMID12202584.
- ^Niobe-Eyangoh SN, Kuaban C, Sorlin P, Cunin P, Thonnon J, Sola C, et al. (June 2003)."Genetic biodiversity of Mycobacterium tuberculosis complex strains from patients with pulmonary tuberculosis in Cameroon".Journal of Clinical Microbiology.41(6): 2547–53.doi:10.1128/JCM.41.6.2547-2553.2003.PMC156567.PMID12791879.
- ^Thoen C, Lobue P, de Kantor I (February 2006). "The importance of Mycobacterium bovis as a zoonosis".Veterinary Microbiology.112(2–4): 339–45.doi:10.1016/j.vetmic.2005.11.047.PMID16387455.
- ^Acton QA (2011).Mycobacterium Infections: New Insights for the Healthcare Professional.ScholarlyEditions. p. 1968.ISBN978-1-4649-0122-5.Archivedfrom the original on 6 September 2015.
- ^Pfyffer GE, Auckenthaler R, van Embden JD, van Soolingen D (1998)."Mycobacterium canettii, the smooth variant of M. tuberculosis, isolated from a Swiss patient exposed in Africa".Emerging Infectious Diseases.4(4): 631–4.doi:10.3201/eid0404.980414.PMC2640258.PMID9866740.
- ^Panteix G, Gutierrez MC, Boschiroli ML, Rouviere M, Plaidy A, Pressac D, et al. (August 2010)."Pulmonary tuberculosis due to Mycobacterium microti: a study of six recent cases in France".Journal of Medical Microbiology.59(Pt 8): 984–989.doi:10.1099/jmm.0.019372-0.PMID20488936.
- ^American Thoracic Society (August 1997). "Diagnosis and treatment of disease caused by nontuberculous mycobacteria".American Journal of Respiratory and Critical Care Medicine.156(2 Pt 2): S1–25.doi:10.1164/ajrccm.156.2.atsstatement.PMID9279284.
- ^Cole EC, Cook CE (August 1998)."Characterization of infectious aerosols in health care facilities: an aid to effective engineering controls and preventive strategies".American Journal of Infection Control.26(4): 453–64.doi:10.1016/S0196-6553(98)70046-X.PMC7132666.PMID9721404.
- ^Nicas M, Nazaroff WW, Hubbard A (March 2005)."Toward understanding the risk of secondary airborne infection: emission of respirable pathogens".Journal of Occupational and Environmental Hygiene.2(3): 143–54.doi:10.1080/15459620590918466.PMC7196697.PMID15764538.
- ^abAhmed N, Hasnain SE (September 2011). "Molecular epidemiology of tuberculosis in India: moving forward with a systems biology approach".Tuberculosis.91(5): 407–13.doi:10.1016/j.tube.2011.03.006.PMID21514230.
- ^ab"Tuberculosis Fact sheet N°104".World Health Organization(WHO). November 2010.Archivedfrom the original on 4 October 2006.Retrieved26 July2011.
- ^ab"Core Curriculum on Tuberculosis: What the Clinician Should Know"(PDF)(5th ed.).Centers for Disease Control and Prevention(CDC), Division of Tuberculosis Elimination. 2011. p. 24.Archived(PDF)from the original on 19 May 2012.
- ^"Causes of Tuberculosis".Mayo Clinic.21 December 2006.Archivedfrom the original on 18 October 2007.Retrieved19 October2007.
- ^abcdeNarasimhan P, Wood J, Macintyre CR, Mathai D (2013)."Risk factors for tuberculosis".Pulmonary Medicine.2013:828939.doi:10.1155/2013/828939.PMC3583136.PMID23476764.
- ^abc"The sixteenth global report on tuberculosis"(PDF).World Health Organization (WHO). 2011. Archived fromthe original(PDF)on 6 September 2012.
- ^"Global tuberculosis control–surveillance, planning, financing WHO Report 2006".World Health Organization (WHO).Archivedfrom the original on 12 December 2006.Retrieved13 October2006.
- ^Chaisson RE, Martinson NA (March 2008)."Tuberculosis in Africa – combating an HIV-driven crisis".The New England Journal of Medicine.358(11): 1089–92.doi:10.1056/NEJMp0800809.PMID18337598.
- ^Restrepo BI (August 2007)."Convergence of the tuberculosis and diabetes epidemics: renewal of old acquaintances".Clinical Infectious Diseases.45(4): 436–438.doi:10.1086/519939.PMC2900315.PMID17638190.
- ^"Targeted tuberculin testing and treatment of latent tuberculosis infection. American Thoracic Society".MMWR. Recommendations and Reports.49(RR-6): 1–51. June 2000.PMID10881762.Archivedfrom the original on 17 December 2004.
- ^van Zyl Smit RN, Pai M, Yew WW, Leung CC, Zumla A, Bateman ED, et al. (January 2010)."Global lung health: the colliding epidemics of tuberculosis, tobacco smoking, HIV and COPD".The European Respiratory Journal.35(1): 27–33.doi:10.1183/09031936.00072909.PMC5454527.PMID20044459.
These analyses indicate that smokers are almost twice as likely to be infected with TB and to progress to active disease (RR of about 1.5 for latent TB infection (LTBI) and RR of ~2.0 for TB disease). Smokers are also twice as likely to die from TB (RR of about 2.0 for TB mortality), but data are difficult to interpret because of heterogeneity in the results across studies.
- ^"TB Risk Factors".CDC.18 March 2016.Archivedfrom the original on 30 August 2020.Retrieved25 August2020.
- ^Möller M, Hoal EG (March 2010). "Current findings, challenges and novel approaches in human genetic susceptibility to tuberculosis".Tuberculosis.90(2): 71–83.doi:10.1016/j.tube.2010.02.002.PMID20206579.
- ^Good JM, Cooper S, Doane AS (1835).The Study of Medicine.Harper. p. 32.Archivedfrom the original on 10 August 2016.
- ^abSkolnik R (2011).Global health 101(2nd ed.). Burlington, MA: Jones & Bartlett Learning. p.253.ISBN978-0-7637-9751-5.
- ^abMainous III AR, Pomeroy C (2009).Management of antimicrobials in infectious diseases: impact of antibiotic resistance(2nd rev. ed.). Totowa, NJ: Humana Press. p. 74.ISBN978-1-60327-238-4.Archivedfrom the original on 6 September 2015.
- ^Houben EN, Nguyen L, Pieters J (February 2006). "Interaction of pathogenic mycobacteria with the host immune system".Current Opinion in Microbiology.9(1): 76–85.doi:10.1016/j.mib.2005.12.014.PMID16406837.
- ^Queval CJ, Brosch R, Simeone R (2017)."Mycobacterium tuberculosis".Frontiers in Microbiology.8:2284.doi:10.3389/fmicb.2017.02284.PMC5703847.PMID29218036.
- ^Khan MR (2011).Essence of Paediatrics.Elsevier India. p. 401.ISBN978-81-312-2804-3.Archivedfrom the original on 6 September 2015.
- ^Herrmann JL, Lagrange PH (February 2005). "Dendritic cells and Mycobacterium tuberculosis: which is the Trojan horse?".Pathologie-Biologie.53(1): 35–40.doi:10.1016/j.patbio.2004.01.004.PMID15620608.
- ^Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D (April 2005)."Tuberculous dilated cardiomyopathy: an under-recognized entity?".BMC Infectious Diseases.5(1): 29.doi:10.1186/1471-2334-5-29.PMC1090580.PMID15857515.
- ^abcdGrosset J (March 2003)."Mycobacterium tuberculosis in the extracellular compartment: an underestimated adversary".Antimicrobial Agents and Chemotherapy.47(3): 833–36.doi:10.1128/AAC.47.3.833-836.2003.PMC149338.PMID12604509.
- ^Bozzano F, Marras F, De Maria A (2014)."Immunology of tuberculosis".Mediterranean Journal of Hematology and Infectious Diseases.6(1): e2014027.doi:10.4084/MJHID.2014.027.PMC4010607.PMID24804000.
- ^Crowley LV (2010).An introduction to human disease: pathology and pathophysiology correlations(8th ed.). Sudbury, MA: Jones and Bartlett. p. 374.ISBN978-0-7637-6591-0.Archivedfrom the original on 6 September 2015.
- ^Harries AD, Maher D, Graham S (2005).TB/HIV a Clinical Manual(2nd ed.). Geneva: World Health Organization (WHO). p. 75.ISBN978-92-4-154634-8.Archivedfrom the original on 6 September 2015.
- ^Jacob JT, Mehta AK, Leonard MK (January 2009). "Acute forms of tuberculosis in adults".The American Journal of Medicine.122(1): 12–17.doi:10.1016/j.amjmed.2008.09.018.PMID19114163.
- ^abBento J, Silva AS, Rodrigues F, Duarte R (2011)."[Diagnostic tools in tuberculosis]".Acta Médica Portuguesa.24(1): 145–54.doi:10.20344/amp.333.PMID21672452.S2CID76156550.
- ^abcdEscalante P (June 2009). "In the clinic. Tuberculosis".Annals of Internal Medicine.150(11): ITC61-614, quiz ITV616.doi:10.7326/0003-4819-150-11-200906020-01006.PMID19487708.S2CID639982.
- ^Metcalfe JZ, Everett CK, Steingart KR, Cattamanchi A, Huang L, Hopewell PC, et al. (November 2011)."Interferon-γ release assays for active pulmonary tuberculosis diagnosis in adults in low- and middle-income countries: systematic review and meta-analysis".The Journal of Infectious Diseases.204(suppl_4): S1120-9.doi:10.1093/infdis/jir410.PMC3192542.PMID21996694.
- ^abSester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB, et al. (January 2011)."Interferon-γ release assays for the diagnosis of active tuberculosis: a systematic review and meta-analysis".The European Respiratory Journal.37(1): 100–11.doi:10.1183/09031936.00114810.PMID20847080.
- ^Chen J, Zhang R, Wang J, Liu L, Zheng Y, Shen Y, et al. (2011).Vermund SH(ed.)."Interferon-gamma release assays for the diagnosis of active tuberculosis in HIV-infected patients: a systematic review and meta-analysis".PLOS ONE.6(11): e26827.Bibcode:2011PLoSO...626827C.doi:10.1371/journal.pone.0026827.PMC3206065.PMID22069472.
- ^Special Programme for Research & Training in Tropical Diseases (2006).Diagnostics for tuberculosis: global demand and market potential.Geneva: World Health Organization (WHO). p. 36.ISBN978-92-4-156330-7.Archivedfrom the original on 6 September 2015.
- ^abNational Institute for Health and Clinical Excellence.Clinical guideline 117: Tuberculosis.London, 2011.
- ^Steingart KR, Flores LL, Dendukuri N, Schiller I, Laal S, Ramsay A, et al. (August 2011). Evans C (ed.)."Commercial serological tests for the diagnosis of active pulmonary and extrapulmonary tuberculosis: an updated systematic review and meta-analysis".PLOS Medicine.8(8): e1001062.doi:10.1371/journal.pmed.1001062.PMC3153457.PMID21857806.
- ^Rothel JS, Andersen P (December 2005). "Diagnosis of latent Mycobacterium tuberculosis infection: is the demise of the Mantoux test imminent?".Expert Review of Anti-Infective Therapy.3(6): 981–93.doi:10.1586/14787210.3.6.981.PMID16307510.S2CID25423684.
- ^Pai M, Zwerling A, Menzies D (August 2008)."Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update".Annals of Internal Medicine.149(3): 177–84.doi:10.7326/0003-4819-149-3-200808050-00241.PMC2951987.PMID18593687.
- ^Jindal SK, ed. (2011).Textbook of Pulmonary and Critical Care Medicine.New Delhi: Jaypee Brothers Medical Publishers. p. 544.ISBN978-93-5025-073-0.Archivedfrom the original on 6 September 2015.
- ^Amicosante M, Ciccozzi M, Markova R (April 2010). "Rational use of immunodiagnostic tools for tuberculosis infection: guidelines and cost effectiveness studies".The New Microbiologica.33(2): 93–107.PMID20518271.
- ^Bibbins-Domingo K, Grossman DC, Curry SJ, Bauman L, Davidson KW, Epling JW, et al. (September 2016)."Screening for Latent Tuberculosis Infection in Adults: US Preventive Services Task Force Recommendation Statement".JAMA.316(9): 962–9.doi:10.1001/jama.2016.11046.PMID27599331.
- ^Gill J, Prasad V (November 2019)."Testing Healthcare Workers for Latent Tuberculosis: Is It Evidence Based, Bio-Plausible, Both, Or Neither?".The American Journal of Medicine.132(11): 1260–1261.doi:10.1016/j.amjmed.2019.03.017.PMID30946831.
- ^Sosa LE, Njie GJ, Lobato MN, Bamrah Morris S, Buchta W, Casey ML, et al. (May 2019)."Tuberculosis Screening, Testing, and Treatment of U.S. Health Care Personnel: Recommendations from the National Tuberculosis Controllers Association and CDC, 2019".MMWR. Morbidity and Mortality Weekly Report.68(19): 439–443.doi:10.15585/mmwr.mm6819a3.PMC6522077.PMID31099768.
- ^Coker R, Thomas M, Lock K, Martin R (2007). "Detention and the evolving threat of tuberculosis: evidence, ethics, and law".The Journal of Law, Medicine & Ethics.35(4): 609–15, 512.doi:10.1111/j.1748-720X.2007.00184.x.PMID18076512.S2CID19924571.
- ^McShane H (October 2011)."Tuberculosis vaccines: beyond bacille Calmette-Guerin".Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences.366(1579): 2782–89.doi:10.1098/rstb.2011.0097.PMC3146779.PMID21893541.
- ^"Vaccines | Basic TB Facts".CDC. 16 June 2021.Archivedfrom the original on 30 December 2021.Retrieved30 December2021.
- ^Roy A, Eisenhut M, Harris RJ, Rodrigues LC, Sridhar S, Habermann S, et al. (August 2014)."Effect of BCG vaccination against Mycobacterium tuberculosis infection in children: systematic review and meta-analysis".BMJ.349(aug04 5): g4643.doi:10.1136/bmj.g4643.PMC4122754.PMID25097193.
- ^Dias JV, Varandas L, Gonçalves L, Kagina B (1 June 2024)."Outcomes of childhood TB in countries with a universal BCG vaccination policy".The International Journal of Tuberculosis and Lung Disease: The Official Journal of the International Union Against Tuberculosis and Lung Disease.28(6): 273–277.doi:10.5588/ijtld.23.0321.ISSN1815-7920.PMID38822485.
- ^"Vaccine and Immunizations: TB Vaccine (BCG)".Centers for Disease Control and Prevention. 2011. Archived fromthe originalon 17 November 2011.Retrieved26 July2011.
- ^"BCG Vaccine Usage in Canada – Current and Historical".Public Health Agency of Canada.September 2010. Archived fromthe originalon 30 March 2012.Retrieved30 December2011.
- ^abTeo SS, Shingadia DV (June 2006)."Does BCG have a role in tuberculosis control and prevention in the United Kingdom?".Archives of Disease in Childhood.91(6): 529–31.doi:10.1136/adc.2005.085043.PMC2082765.PMID16714729.
- ^Kashangura R, Jullien S, Garner P, Johnson S, et al. (Cochrane Infectious Diseases Group) (April 2019)."MVA85A vaccine to enhance BCG for preventing tuberculosis".The Cochrane Database of Systematic Reviews.2019(4): CD012915.doi:10.1002/14651858.CD012915.pub2.PMC6488980.PMID31038197.
- ^Clark M, Riben P, Nowgesic E (October 2002)."The association of housing density, isolation and tuberculosis in Canadian First Nations communities".International Journal of Epidemiology.31(5): 940–945.doi:10.1093/ije/31.5.940.PMID12435764.
- ^Barberis I, Bragazzi NL, Galluzzo L, Martini M (March 2017)."The history of tuberculosis: from the first historical records to the isolation of Koch's bacillus".Journal of Preventive Medicine and Hygiene.58(1): E9–E12.PMC5432783.PMID28515626.
- ^"Introduction".Tuberculosis in the Workplace.National Academies Press (US). 2001.
- ^"Basics of Tuberculosis.".Tuberculosis in the Workplace.National Academies Press (US). 2001.
- ^"DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention Guidelines for Preventing the Transmission of Mycobacterium Tuberculosis in Health-Care Facilities, 1994"(PDF).US Federal Register.Retrieved8 May2024.
- ^"DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service 42 CFR Part 84"(PDF).US Federal Register. pp. 26850-26893.Retrieved8 May2024.
- ^"Introduction".Introduction. Tuberculosis in the Workplace.National Academies Press (US). 2001.
- ^"DEPARTMENT OF LABOR Occupational Safety and Health Administration 29 CFR Part 1910 [Docket No. H-371] RIN 1218-AB46 Occupational Exposure to Tuberculosis".
- ^"Part III DEPARTMENT OF LABOR Occupational Safety and Health Administration 29 CFR Part 1910 [Docket No. H-371] RIN 1218-AB46 Occupational Exposure to Tuberculosis".
- ^"The Global Plan to Stop TB".World Health Organization(WHO). 2011.Archivedfrom the original on 12 June 2011.Retrieved13 June2011.
- ^Warrell DA, Cox TM, Firth JD, Benz EJ (2005).Sections 1–10(4. ed., paperback ed.). Oxford [u.a.]: Oxford Univ. Press. p. 560.ISBN978-0-19-857014-1.Archivedfrom the original on 6 September 2015.
- ^Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. (May 2015). "WHO's new end TB strategy".Lancet.385(9979): 1799–1801.doi:10.1016/S0140-6736(15)60570-0.PMID25814376.S2CID39379915.
- ^Fraser A, Paul M, Attamna A, Leibovici L, et al. (Cochrane Infectious Diseases Group) (April 2006)."Drugs for preventing tuberculosis in people at risk of multiple-drug-resistant pulmonary tuberculosis".The Cochrane Database of Systematic Reviews.2006(2): CD005435.doi:10.1002/14651858.CD005435.pub2.PMC6532726.PMID16625639.
- ^Piggott DA, Karakousis PC (27 December 2010)."Timing of antiretroviral therapy for HIV in the setting of TB treatment".Clinical & Developmental Immunology.2011:103917.doi:10.1155/2011/103917.PMC3017895.PMID21234380.
- ^Brennan PJ, Nikaido H (1995). "The envelope of mycobacteria".Annual Review of Biochemistry.64(1): 29–63.doi:10.1146/annurev.bi.64.070195.000333.PMID7574484.
- ^Davies G, Cerri S, Richeldi L (October 2007)."Rifabutin for treating pulmonary tuberculosis".The Cochrane Database of Systematic Reviews.2007(4): CD005159.doi:10.1002/14651858.CD005159.pub2.PMC6532710.PMID17943842.
- ^Di Bella S, Luzzati R, Principe L, Zerbato V, Meroni E, Giuffrè M, et al. (January 2022)."Aspirin and Infection: A Narrative Review".Biomedicines.10(2): 263.doi:10.3390/biomedicines10020263.PMC8868581.PMID35203473.
- ^abLatent tuberculosis infection.World Health Organization(WHO). 2018. p. 23.ISBN978-92-4-155023-9.Archivedfrom the original on 2 June 2021.Retrieved25 July2018.
- ^Borisov AS, Bamrah Morris S, Njie GJ, Winston CA, Burton D, Goldberg S, et al. (June 2018)."Update of Recommendations for Use of Once-Weekly Isoniazid-Rifapentine Regimen to Treat Latent Mycobacterium tuberculosis Infection".MMWR. Morbidity and Mortality Weekly Report.67(25): 723–726.doi:10.15585/mmwr.mm6725a5.PMC6023184.PMID29953429.
- ^abSterling TR, Njie G, Zenner D, Cohn DL, Reves R, Ahmed A, et al. (February 2020)."Guidelines for the Treatment of Latent Tuberculosis Infection: Recommendations from the National Tuberculosis Controllers Association and CDC, 2020".MMWR. Recommendations and Reports.69(1): 1–11.doi:10.15585/mmwr.rr6901a1.PMC7041302.PMID32053584.
- ^Njie GJ, Morris SB, Woodruff RY, Moro RN, Vernon AA, Borisov AS (August 2018)."Isoniazid-Rifapentine for Latent Tuberculosis Infection: A Systematic Review and Meta-analysis".American Journal of Preventive Medicine.55(2): 244–252.doi:10.1016/j.amepre.2018.04.030.PMC6097523.PMID29910114.
- ^Menzies D, Al Jahdali H, Al Otaibi B (March 2011)."Recent developments in treatment of latent tuberculosis infection".The Indian Journal of Medical Research.133(3): 257–66.PMC3103149.PMID21441678.
- ^M'imunya JM, Kredo T, Volmink J, et al. (Cochrane Infectious Diseases Group) (May 2012)."Patient education and counselling for promoting adherence to treatment for tuberculosis".The Cochrane Database of Systematic Reviews.2012(5): CD006591.doi:10.1002/14651858.CD006591.pub2.PMC6532681.PMID22592714.
- ^Gelband H, et al. (Cochrane Infectious Diseases Group) (25 October 1999)."Regimens of less than six months for treating tuberculosis".The Cochrane Database of Systematic Reviews.1999(2): CD001362.doi:10.1002/14651858.CD001362.PMC6532732.PMID10796641.
- ^Grace AG, Mittal A, Jain S, Tripathy JP, Satyanarayana S, Tharyan P, et al. (Cochrane Infectious Diseases Group) (December 2019)."Shortened treatment regimens versus the standard regimen for drug-sensitive pulmonary tuberculosis".The Cochrane Database of Systematic Reviews.12(12): CD012918.doi:10.1002/14651858.CD012918.pub2.PMC6953336.PMID31828771.
- ^"Landmark TB Trial Identifies Shorter-Course Treatment Regimen".CDC.NCHHSTP Media Team Centers for Disease Control and Prevention. 20 October 2020.Archivedfrom the original on 27 November 2021.Retrieved27 November2021.
- ^Mainous III AB (2010).Management of Antimicrobials in Infectious Diseases: Impact of Antibiotic Resistance.Totowa, NJ: Humana Press. p. 69.ISBN978-1-60327-238-4.Archivedfrom the original on 6 September 2015.
- ^abcKarumbi J, Garner P (May 2015)."Directly observed therapy for treating tuberculosis".The Cochrane Database of Systematic Reviews.2015(5): CD003343.doi:10.1002/14651858.CD003343.pub4.PMC4460720.PMID26022367.
- ^Liu Q, Abba K, Alejandria MM, Sinclair D, Balanag VM, Lansang MA, et al. (Cochrane Infectious Diseases Group) (November 2014)."Reminder systems to improve patient adherence to tuberculosis clinic appointments for diagnosis and treatment".The Cochrane Database of Systematic Reviews.2014(11): CD006594.doi:10.1002/14651858.CD006594.pub3.PMC4448217.PMID25403701.
- ^Mwandumba HC, Squire SB, et al. (Cochrane Infectious Diseases Group) (23 October 2001)."Fully intermittent dosing with drugs for treating tuberculosis in adults".The Cochrane Database of Systematic Reviews(4): CD000970.doi:10.1002/14651858.CD000970.PMC6532565.PMID11687088.
- ^Bose A, Kalita S, Rose W, Tharyan P, et al. (Cochrane Infectious Diseases Group) (January 2014)."Intermittent versus daily therapy for treating tuberculosis in children".The Cochrane Database of Systematic Reviews.2014(1): CD007953.doi:10.1002/14651858.CD007953.pub2.PMC6532685.PMID24470141.
- ^O'Brien RJ (June 1994). "Drug-resistant tuberculosis: etiology, management and prevention".Seminars in Respiratory Infections.9(2): 104–12.PMID7973169.
- ^Centers for Disease Control and Prevention (CDC) (March 2006)."Emergence of Mycobacterium tuberculosis with extensive resistance to second-line drugs—worldwide, 2000–2004".MMWR. Morbidity and Mortality Weekly Report.55(11): 301–5.PMID16557213.Archivedfrom the original on 22 May 2017.
- ^abMcKenna M (12 January 2012)."Totally Resistant TB: Earliest Cases in Italy".Wired.Archivedfrom the original on 14 January 2012.Retrieved12 January2012.
- ^Migliori GB, De Iaco G, Besozzi G, Centis R, Cirillo DM (May 2007)."First tuberculosis cases in Italy resistant to all tested drugs".Euro Surveillance.12(5): E070517.1.doi:10.2807/esw.12.20.03194-en.PMID17868596.
- ^"Totally Drug-Resistant TB: a WHO consultation on the diagnostic definition and treatment options"(PDF).World Health Organization (WHO).Archived(PDF)from the original on 21 October 2016.Retrieved25 March2016.
- ^abcdefghijklmnopKielstra P (30 June 2014). Tabary Z (ed.)."Ancient enemy, modern imperative – A time for greater action against tuberculosis"(PDF).The Economist.Economist Intelligence Unit.Archived fromthe original(PDF)on 10 August 2014.Retrieved22 January2022.
- ^Singh B, Cocker D, Ryan H, Sloan DJ, et al. (Cochrane Infectious Diseases Group) (March 2019)."Linezolid for drug-resistant pulmonary tuberculosis".The Cochrane Database of Systematic Reviews.3(3): CD012836.doi:10.1002/14651858.CD012836.pub2.PMC6426281.PMID30893466.
- ^Velayati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, ZiaZarifi AH, et al. (August 2009). "Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in Iran".Chest.136(2): 420–425.doi:10.1378/chest.08-2427.PMID19349380.
- ^"Provisional CDC Guidelines for the Use and Safety Monitoring of Bedaquiline Fumarate (Sirturo) for the Treatment of Multidrug-Resistant Tuberculosis".Archivedfrom the original on 4 January 2014.
- ^Theron G, Peter J, Richardson M, Warren R, Dheda K, Steingart KR, et al. (Cochrane Infectious Diseases Group) (September 2016)."® MTBDRsl assay for resistance to second-line anti-tuberculosis drugs".The Cochrane Database of Systematic Reviews.2016(9): CD010705.doi:10.1002/14651858.CD010705.pub3.PMC5034505.PMID27605387.
- ^"The use of molecular line probe assays for the detection of resistance to second-line anti-tuberculosis drugs"(PDF).World Health Organization.Archived(PDF)from the original on 22 September 2021.Retrieved18 June2021.
- ^"WHO Disease and injury country estimates".World Health Organization (WHO). 2004.Archivedfrom the original on 11 November 2009.Retrieved11 November2009.
- ^Lambert ML, Hasker E, Van Deun A, Roberfroid D, Boelaert M, Van der Stuyft P (May 2003). "Recurrence in tuberculosis: relapse or reinfection?".The Lancet. Infectious Diseases.3(5): 282–7.doi:10.1016/S1473-3099(03)00607-8.PMID12726976.
- ^Wang JY, Lee LN, Lai HC, Hsu HL, Liaw YS, Hsueh PR, et al. (July 2007)."Prediction of the tuberculosis reinfection proportion from the local incidence".The Journal of Infectious Diseases.196(2): 281–8.doi:10.1086/518898.PMID17570116.
- ^"1.4 Prognosis – Tuberculosis".medicalguidelines.msf.org.Archivedfrom the original on 2 June 2021.Retrieved25 August2020.
- ^"Fact Sheets: The Difference Between Latent TB Infection and Active TB Disease".Centers for Disease Control and Prevention(CDC). 20 June 2011.Archivedfrom the original on 4 August 2011.Retrieved26 July2011.
- ^"Global tuberculosis report 2013".World Health Organization (WHO). 2013.Archivedfrom the original on 12 December 2006.
- ^Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. (December 2012)."Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010".Lancet.380(9859): 2095–128.doi:10.1016/S0140-6736(12)61728-0.hdl:10536/DRO/DU:30050819.PMC10790329.PMID23245604.S2CID1541253.Archivedfrom the original on 19 May 2020.Retrieved18 March2020.
- ^abc"Global Tuberculosis Control 2011"(PDF).World Health Organization (WHO). Archived fromthe original(PDF)on 17 June 2012.Retrieved15 April2012.
- ^"Tuberculosis".WHO.24 March 2020.Archivedfrom the original on 30 July 2020.Retrieved31 May2020.
- ^Douglas AS, Strachan DP, Maxwell JD (September 1996)."Seasonality of tuberculosis: the reverse of other respiratory diseases in the UK".Thorax.51(9): 944–946.doi:10.1136/thx.51.9.944.PMC472621.PMID8984709.
- ^Martineau AR, Nhamoyebonde S, Oni T, Rangaka MX, Marais S, Bangani N, et al. (November 2011)."Reciprocal seasonal variation in vitamin D status and tuberculosis notifications in Cape Town, South Africa".Proceedings of the National Academy of Sciences of the United States of America.108(47): 19013–19017.doi:10.1073/pnas.1111825108.PMC3223428.PMID22025704.
- ^Parrinello CM, Crossa A, Harris TG (January 2012). "Seasonality of tuberculosis in New York City, 1990-2007".The International Journal of Tuberculosis and Lung Disease.16(1): 32–37.doi:10.5588/ijtld.11.0145.PMID22236842.
- ^abKorthals Altes H, Kremer K, Erkens C, van Soolingen D, Wallinga J (May 2012). "Tuberculosis seasonality in the Netherlands differs between natives and non-natives: a role for vitamin D deficiency?".The International Journal of Tuberculosis and Lung Disease.16(5): 639–644.doi:10.5588/ijtld.11.0680.PMID22410705.
- ^Koh GC, Hawthorne G, Turner AM, Kunst H, Dedicoat M (2013)."Tuberculosis incidence correlates with sunshine: an ecological 28-year time series study".PLOS ONE.8(3): e57752.Bibcode:2013PLoSO...857752K.doi:10.1371/journal.pone.0057752.PMC3590299.PMID23483924.
- ^Kuddus MA, McBryde ES, Adegboye OA (September 2019)."Delay effect and burden of weather-related tuberculosis cases in Rajshahi province, Bangladesh, 2007–2012".Scientific Reports.9(1): 12720.Bibcode:2019NatSR...912720K.doi:10.1038/s41598-019-49135-8.PMC6722246.PMID31481739.
- ^Griffith DE, Kerr CM (August 1996). "Tuberculosis: disease of the past, disease of the present".Journal of PeriAnesthesia Nursing.11(4): 240–45.doi:10.1016/S1089-9472(96)80023-2.PMID8964016.
- ^"Global Tuberculosis Control Report, 2006 – Annex 1 Profiles of high-burden countries"(PDF).World Health Organization (WHO). Archived fromthe original(PDF)on 26 July 2009.Retrieved13 October2006.
- ^"2005 Surveillance Slide Set".Centers for Disease Control and Prevention. 12 September 2006.Archivedfrom the original on 23 November 2006.Retrieved13 October2006.
- ^FitzGerald JM, Wang L, Elwood RK (February 2000)."Tuberculosis: 13. Control of the disease among aboriginal people in Canada".Canadian Medical Association Journal.162(3): 351–55.PMC1231016.PMID10693593.
- ^Quah SR, Carrin G, Buse K, Heggenhougen K (2009).Health Systems Policy, Finance, and Organization.Boston: Academic Press. p. 424.ISBN978-0-12-375087-7.Archivedfrom the original on 6 September 2015.
- ^"Origins of the MRC".Medical Research Council.Archived fromthe originalon 11 April 2008.Retrieved7 October2006.
- ^"Global Tuberculosis Report 2024".www.who.int.Retrieved31 October2024.
- ^"WHO report shows global tuberculosis cases are rising | CIDRAP".www.cidrap.umn.edu.29 October 2024.Retrieved31 October2024.
- ^Shkolnikov VM, Meslé F (1996). "The Russian Epidemiological Crisis as Mirrored by Mortality Trends". In DaVanzo J, Farnsworth G (eds.).Russia's Demographic "Crisis".RAND Corporation. p. 142.ISBN0-8330-2446-9.Archivedfrom the original on 20 February 2023.Retrieved20 February2023.
- ^"Global Tuberculosis Control".World Health Organization. 2011. Archived fromthe originalon 12 December 2006.
- ^"WHO global tuberculosis report 2016. Annex 2. Country profiles: Russian Federation".Archived fromthe originalon 14 July 2017.Retrieved22 August2020.
- ^ab"Global Tuberculosis Report 2018"(PDF).Archived(PDF)from the original on 7 August 2020.Retrieved27 September2019.
- ^Tomlinson C (10 November 2023)."In-depth: What new WHO TB numbers mean for South Africa".Spotlight.Retrieved27 March2024.
- ^"WHO Global tuberculosis report 2016: India".Archived fromthe originalon 6 February 2018.Retrieved22 August2020.
- ^"Govt revisits strategy to combat tuberculosis".Daily News and Analysis.8 April 2017.Archivedfrom the original on 3 June 2021.Retrieved22 August2020.
- ^Mahla RS (August 2018)."Prevalence of drug-resistant tuberculosis in South Africa".The Lancet. Infectious Diseases.18(8): 836.doi:10.1016/S1473-3099(18)30401-8.PMID30064674.
- ^Al-Azem A, Kaushal Sharma M, Turenne C, Hoban D, Hershfield E, MacMorran J, et al. (1998)."Rural outbreaks ofMycobacterium tuberculosisin a Canadian province ".Abstr Intersci Conf Antimicrob Agents Chemother.38:555. abstract no. L-27. Archived fromthe originalon 18 November 2011.
- ^"Tuberculosis (TB): Monitoring".Government of Canada. 4 March 2024.Archivedfrom the original on 26 March 2024.Retrieved30 October2024.
- ^Birn AE (2009).Textbook of International Health: Global Health in a Dynamic World.Oxford University Press. p. 261.ISBN978-0-19-988521-3.Archivedfrom the original on 6 September 2015.
- ^abWilliams PM, Pratt RH, Walker WL, Price SF, Stewart RJ, Feng PI."Tuberculosis — United States, 2023".MMWR. Morbidity and Mortality Weekly Report.73(12): 265–270.doi:10.15585/mmwr.mm7312a4.PMC10986816.
- ^Bendix A (7 May 2024)."California city declares a public health emergency after tuberculosis sickens 14".NBC News.
- ^"Tuberculosis incidence (per 100,000 people)".Our World in Data.Archivedfrom the original on 26 September 2019.Retrieved7 March2020.
- ^"Tuberculosis deaths by region".Our World in Data.Archivedfrom the original on 8 May 2020.Retrieved7 March2020.
- ^abcLawlor C."Katherine Byrne, Tuberculosis and the Victorian Literary Imagination".British Society for Literature and Science.Archivedfrom the original on 6 November 2020.Retrieved11 June2017.
- ^"Hippocrates 3.16 Classics, MIT".Archived fromthe originalon 11 February 2005.Retrieved15 December2015.
- ^Caldwell M (1988).The Last Crusade.New York: Macmillan. p.21.ISBN978-0-689-11810-4.
- ^Bunyan J (1808).The Life and Death of Mr. Badman.London: W. Nicholson. p.244.Retrieved28 September2016– via Internet Archive.
captain.
- ^Byrne K (2011).Tuberculosis and the Victorian Literary Imagination.Cambridge University Press.ISBN978-1-107-67280-2.
- ^"About Chopin's illness".Icons of Europe.Archivedfrom the original on 28 September 2017.Retrieved11 June2017.
- ^Vilaplana C (March 2017)."A literary approach to tuberculosis: lessons learned from Anton Chekhov, Franz Kafka, and Katherine Mansfield".International Journal of Infectious Diseases.56:283–85.doi:10.1016/j.ijid.2016.12.012.PMID27993687.
- ^Rogal SJ (1997).A William Somerset Maugham Encyclopedia.Greenwood Publishing. p. 245.ISBN978-0-313-29916-2.Archivedfrom the original on 2 June 2021.Retrieved4 October2017.
- ^Eschner K."George Orwell Wrote '1984' While Dying of Tuberculosis".Smithsonian.Archivedfrom the original on 24 March 2019.Retrieved25 March2019.
- ^"Tuberculosis (whole issue)".Journal of the American Medical Association.293(22): cover. 8 June 2005.Archivedfrom the original on 24 August 2020.Retrieved4 October2017.
- ^Lemlein RF (1981). "Influence of Tuberculosis on the Work of Visual Artists: Several Prominent Examples".Leonardo.14(2): 114–11.doi:10.2307/1574402.JSTOR1574402.S2CID191371443.
- ^Wilsey AM (May 2012).'Half in Love with Easeful Death:' Tuberculosis in Literature.Humanities Capstone Projects(PhD Thesis thesis). Pacific University. Archived fromthe originalon 11 October 2017.Retrieved28 September2017.
- ^abMorens DM (November 2002)."At the deathbed of consumptive art".Emerging Infectious Diseases.8(11): 1353–8.doi:10.3201/eid0811.020549.PMC2738548.PMID12463180.
- ^"Pulmonary Tuberculosis/In Literature and Art".McMaster University History of Diseases.Retrieved9 June2017.
- ^Thomson G (1 June 2016)."Van Morrison – 10 of the best".The Guardian.Archivedfrom the original on 14 August 2020.Retrieved28 September2017.
- ^"Tuberculosis Throughout History: The Arts"(PDF).United States Agency for International Development(USAID).Archived(PDF)from the original on 30 June 2017.Retrieved12 June2017.
- ^Corliss R (22 December 2008)."Top 10 Worst Christmas Movies".Time.Archivedfrom the original on 22 September 2020.Retrieved28 September2017.
'If you don't cry when Bing Crosby tells Ingrid Bergman she has tuberculosis', Joseph McBride wrote in 1973, 'I never want to meet you, and that's that.'
- ^"The End TB Strategy".who.int.Archivedfrom the original on 22 July 2021.Retrieved22 July2021.
- ^abcdGlobal tuberculosis report 2020.World Health Organization. 2020.ISBN978-92-4-001313-1.Archivedfrom the original on 22 July 2021.Retrieved22 July2021.
- ^ab"Public–Private Partnership Announces Immediate 40 Percent Cost Reduction for Rapid TB Test"(PDF).World Health Organization (WHO). 6 August 2012.Archived(PDF)from the original on 29 October 2013.
- ^Lawn SD, Nicol MP (September 2011)."Xpert® MTB/RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance".Future Microbiology.6(9): 1067–82.doi:10.2217/fmb.11.84.PMC3252681.PMID21958145.
- ^"WHO says Cepheid rapid test will transform TB care".Reuters.8 December 2010.Archivedfrom the original on 11 December 2010.
- ^STOPTB (5 April 2013)."The Stop TB Partnership, which operates through a secretariat hosted by the World Health Organization (WHO) in Geneva, Switzerland"(PDF).Archived(PDF)from the original on 24 January 2014.
- ^Lienhardt C, Espinal M, Pai M, Maher D, Raviglione MC (November 2011)."What research is needed to stop TB? Introducing the TB Research Movement".PLOS Medicine.8(11): e1001135.doi:10.1371/journal.pmed.1001135.PMC3226454.PMID22140369.
- ^Sandhu GK (2011)."Tuberculosis: Current Situation, Challenges and Overview of its Control Programs in India".Journal of Global Infectious Diseases.3(2): 143–150.doi:10.4103/0974-777X.81691.ISSN0974-777X.PMC3125027.PMID21731301.
- ^Bhargava A, Pinto L, Pai M (2011)."Mismanagement of tuberculosis in India: Causes, consequences, and the way forward"(PDF).Hypothesis.9(1): e7. Archived fromthe original(PDF)on 24 October 2022.
- ^Amdekar Y (July 2009). "Changes in the management of tuberculosis".Indian Journal of Pediatrics.76(7): 739–42.doi:10.1007/s12098-009-0164-4.PMID19693453.S2CID41788291.
- ^Fox GJ, Dobler CC, Marks GB (September 2011)."Active case finding in contacts of people with tuberculosis".The Cochrane Database of Systematic Reviews.2011(9): CD008477.doi:10.1002/14651858.CD008477.pub2.PMC6532613.PMID21901723.
- ^Mhimbira FA, Cuevas LE, Dacombe R, Mkopi A, Sinclair D, et al. (Cochrane Infectious Diseases Group) (November 2017)."Interventions to increase tuberculosis case detection at primary healthcare or community-level services".The Cochrane Database of Systematic Reviews.2017(11): CD011432.doi:10.1002/14651858.CD011432.pub2.PMC5721626.PMID29182800.
- ^Braganza Menezes D, Menezes B, Dedicoat M, et al. (Cochrane Infectious Diseases Group) (August 2019)."Contact tracing strategies in household and congregate environments to identify cases of tuberculosis in low- and moderate-incidence populations".The Cochrane Database of Systematic Reviews.2019(8): CD013077.doi:10.1002/14651858.CD013077.pub2.PMC6713498.PMID31461540.
- ^abcdefgCourtwright A, Turner AN (July–August 2010)."Tuberculosis and stigmatization: pathways and interventions".Public Health Reports.125(4_suppl): 34–42.doi:10.1177/00333549101250S407.PMC2882973.PMID20626191.
- ^Mason PH, Roy A, Spillane J, Singh P (March 2016)."Social, Historical and Cultural Dimensions of Tuberculosis".Journal of Biosocial Science.48(2): 206–32.doi:10.1017/S0021932015000115.PMID25997539.
- ^abcMartín Montañés C, Gicquel B (March 2011). "New tuberculosis vaccines".Enfermedades Infecciosas y Microbiologia Clinica.29(Suppl 1): 57–62.doi:10.1016/S0213-005X(11)70019-2.PMID21420568.
- ^Zhu B, Dockrell HM, Ottenhoff TH, Evans TG, Zhang Y (April 2018)."Tuberculosis vaccines: Opportunities and challenges".Respirology.23(4): 359–368.doi:10.1111/resp.13245.hdl:1887/77156.PMID29341430.
- ^Ibanga HB, Brookes RH, Hill PC, Owiafe PK, Fletcher HA, Lienhardt C, et al. (August 2006). "Early clinical trials with a new tuberculosis vaccine, MVA85A, in tuberculosis-endemic countries: issues in study design".The Lancet. Infectious Diseases.6(8): 522–8.doi:10.1016/S1473-3099(06)70552-7.PMID16870530.
- ^Kaufmann SH (October 2010)."Future vaccination strategies against tuberculosis: thinking outside the box".Immunity.33(4): 567–77.doi:10.1016/j.immuni.2010.09.015.PMID21029966.
- ^Webber D, Kremer M (2001)."Stimulating Industrial R&D for Neglected Infectious Diseases: Economic Perspectives"(PDF).Bulletin of the World Health Organization.79(8): 693–801.Archived(PDF)from the original on 26 September 2007.
- ^Barder O, Kremer M, Williams H (2006)."Advance Market Commitments: A Policy to Stimulate Investment in Vaccines for Neglected Diseases".The Economists' Voice.3(3).doi:10.2202/1553-3832.1144.S2CID154454583.Archived fromthe originalon 5 November 2006.
- ^Department of Economic and Social Affairs (2009).Achieving the global public health agenda: dialogues at the Economic and Social Council.New York:United Nations.p. 103.ISBN978-92-1-104596-3.Archivedfrom the original on 6 September 2015.
- ^Jong EC, Zuckerman JN (2010).Travelers' vaccines(2nd ed.). Shelton, CT: People's Medical Publishing House. p. 319.ISBN978-1-60795-045-5.Archivedfrom the original on 6 September 2015.
- ^Bill and Melinda Gates Foundation Announcement (12 February 2004)."Gates Foundation Commits $82.9 Million to Develop New Tuberculosis Vaccines".Archived fromthe originalon 10 October 2009.
- ^Nightingale K (19 September 2007)."Gates foundation gives US$280 million to fight TB".Archivedfrom the original on 1 December 2008.
- ^Zumla A, Hafner R, Lienhardt C, Hoelscher M, Nunn A (March 2012)."Advancing the development of tuberculosis therapy".Nature Reviews. Drug Discovery.11(3): 171–172.doi:10.1038/nrd3694.PMID22378254.S2CID7232434.Archivedfrom the original on 12 January 2020.Retrieved8 May2020.
- ^"J&J Sirturo Wins FDA Approval to Treat Drug-Resistant TB".Bloomberg News.31 December 2012.Archivedfrom the original on 4 January 2013.Retrieved1 January2013.
- ^Avorn J (April 2013). "Approval of a tuberculosis drug based on a paradoxical surrogate measure".JAMA.309(13): 1349–1350.doi:10.1001/jama.2013.623.PMID23430122.
- ^US Food and Drug Administration."Briefing Package: NDA 204–384: Sirturo"(PDF).Food and Drug Administration.Archived(PDF)from the original on 4 January 2014.
- ^Zuckerman D, Yttri J (January 2013)."Antibiotics: When science and wishful thinking collide".Health Affairs.doi:10.1377/forefront.20130125.027503.Archivedfrom the original on 29 March 2022.Retrieved29 March2022.
- ^Mbuagbaw L, Guglielmetti L, Hewison C, Bakare N, Bastard M, Caumes E, et al. (May 2019)."Outcomes of Bedaquiline Treatment in Patients with Multidrug-Resistant Tuberculosis".Emerging Infectious Diseases.25(5): 936–943.doi:10.3201/eid2505.181823.PMC6478224.PMID31002070.
- ^abKhoshnood S, Taki E, Sadeghifard N, Kaviar VH, Haddadi MH, Farshadzadeh Z, et al. (7 October 2021)."Mechanism of Action, Resistance, Synergism, and Clinical Implications of Delamanid Against Multidrug-ResistantMycobacterium tuberculosis".Frontiers in Microbiology.12:717045.doi:10.3389/fmicb.2021.717045.PMC8529252.PMID34690963.
- ^"European Medicines Agency – News and Events – European Medicines Agency recommends two new treatment options for tuberculosis".3 December 2013. Archived fromthe originalon 3 December 2013.Retrieved9 April2024.
- ^Critchley JA, Orton LC, Pearson F (November 2014)."Adjunctive steroid therapy for managing pulmonary tuberculosis".The Cochrane Database of Systematic Reviews.2014(11): CD011370.doi:10.1002/14651858.CD011370.PMC6532561.PMID25387839.
- ^Shivaprasad HL, Palmieri C (January 2012). "Pathology of mycobacteriosis in birds".The Veterinary Clinics of North America. Exotic Animal Practice.15(1): 41–55, v–vi.doi:10.1016/j.cvex.2011.11.004.PMID22244112.
- ^Reavill DR, Schmidt RE (January 2012). "Mycobacterial lesions in fish, amphibians, reptiles, rodents, lagomorphs, and ferrets with reference to animal models".The Veterinary Clinics of North America. Exotic Animal Practice.15(1): 25–40, v.doi:10.1016/j.cvex.2011.10.001.PMID22244111.
- ^Mitchell MA (January 2012). "Mycobacterial infections in reptiles".The Veterinary Clinics of North America. Exotic Animal Practice.15(1): 101–11, vii.doi:10.1016/j.cvex.2011.10.002.PMID22244116.
- ^Wobeser GA (2006).Essentials of disease in wild animals(1st ed.). Ames, IO [u.a.]: Blackwell Publishing. p. 170.ISBN978-0-8138-0589-4.Archivedfrom the original on 6 September 2015.
- ^Ryan TJ, Livingstone PG, Ramsey DS, de Lisle GW, Nugent G, Collins DM, et al. (February 2006). "Advances in understanding disease epidemiology and implications for control and eradication of tuberculosis in livestock: the experience from New Zealand".Veterinary Microbiology.112(2–4): 211–19.doi:10.1016/j.vetmic.2005.11.025.PMID16330161.
- ^White PC, Böhm M, Marion G, Hutchings MR (September 2008). "Control of bovine tuberculosis in British livestock: there is no 'silver bullet'".Trends in Microbiology.16(9): 420–7.CiteSeerX10.1.1.566.5547.doi:10.1016/j.tim.2008.06.005.PMID18706814.
- ^Ward AI, Judge J, Delahay RJ (January 2010). "Farm husbandry and badger behaviour: opportunities to manage badger to cattle transmission of Mycobacterium bovis?".Preventive Veterinary Medicine.93(1): 2–10.doi:10.1016/j.prevetmed.2009.09.014.PMID19846226.
- ^Holt N (24 March 2015)."The Infected Elephant in the Room".Slate.Archivedfrom the original on 14 April 2016.Retrieved5 April2016.
- ^Mikota SK."A Brief History of TB in Elephants"(PDF).Animal and Plant Health Inspection Service(APHIS).Archived(PDF)from the original on 6 October 2016.Retrieved5 April2016.
External links
 Definitionsfrom Wiktionary
Definitionsfrom Wiktionary Mediafrom Commons
Mediafrom Commons Quotationsfrom Wikiquote
Quotationsfrom Wikiquote Taxafrom Wikispecies
Taxafrom Wikispecies Datafrom Wikidata
Datafrom Wikidata
- "Tuberculosis (TB)".Centers for Disease Control and Prevention (CDC). 24 October 2018.
- "Tuberculosis (TB)".London:Health Protection Agency.Archived fromthe originalon 5 July 2007.
- WHO global 2016 TB report (infographic)
- WHO tuberculosis country profiles
- "Tuberculosis Among African Americans",1990-11-01,In Black America;KUT Radio,American Archive of Public Broadcasting(WGBHand the Library of Congress)
- Working Group on New TB drugs,tracking clinical trials and drug candidates