This articlemay be too technical for most readers to understand.(May 2015) |
Thesacrospinous ligament(smalloranterior sacrosciatic ligament) is a thin, triangularligamentin thehuman pelvis.The base of the ligament is attached to the outer edge of thesacrumandcoccyx,and the tip of the ligament attaches to thespine of the ischium,a bony protuberance on thehuman pelvis.Its fibres are intermingled with thesacrotuberous ligament.
| Sacrospinous ligament | |
|---|---|
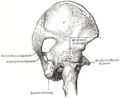
 Articulations of pelvis, anterior view, with greater sciatic foramen (labeled in red) and its boundaries. | |
| Details | |
| From | Ischial spine |
| To | Sacrum |
| Identifiers | |
| Latin | ligamentum sacrospinale |
| TA98 | A03.6.03.007 |
| TA2 | 1852 |
| FMA | 21485 |
| Anatomical terminology | |
Structure
editThesacrotuberous ligamentpasses behind the sacrospinous ligament. In its entire length, the sacrospinous ligament covers the equally triangularcoccygeus muscle,to which its closely connected.[1]
Function
editThe presence of the ligament in thegreater sciatic notchcreates an opening (foramen), thegreater sciatic foramen,and also converts thelesser sciatic notchinto thelesser sciatic foramen.[2]The greater sciatic foramen lies above the ligament, and thelesser sciatic foramenlies below it.
Thepudendal vesselsandnervepass behind the sacrospinous ligament directly medially and inferiorly to the ischial spine. Theinferior gluteal artery,from a branch of theinternal iliac artery,pass behind thesciatic nerveand the sacrospinous ligament and is left uncovered in a small opening above the top of the sacrospinous ligament. The coccygeal branch of the inferior gluteal artery passes behind the mid-portion of the sacrospinous ligament and pierces the sacrotuberous ligament at multiple locations. The main body of the inferior gluteal artery leaves the pelvis posteriorly to the upper border of the sacrospinous ligament, to follow the inferior portion of the sciatic nerve out of the greater sciatic foramen.[3]
The main function of the ligament is to prevent rotation of theiliumpast thesacrum.Laxity of this ligament and the sacrotuberous ligament allows this rotation to occur. Stresses to these ligaments occur most often when leaning forward or getting out of a chair.[citation needed]
Clinical significance
editVaginal prolapseoruterine prolapsemay occur in women when other pelvic ligaments and supportive structures are weakened. One treatment issacrospinous fixation.In this surgery, the apex of thevaginais sutured to the sacrospinous ligament, which may offer a sturdier support than weakened pelvic ligaments, ideally preventing furtherprolapse.[4]
Additional images
edit-
 Nélaton's line and Bryant's triangle.
Nélaton's line and Bryant's triangle. -
 Articulations of pelvis. Posterior view.
Articulations of pelvis. Posterior view.


Notes
editReferences
edit![]() This article incorporates text in thepublic domainfrompage 309of the 20th edition ofGray's Anatomy(1918)
This article incorporates text in thepublic domainfrompage 309of the 20th edition ofGray's Anatomy(1918)
- Thompson, Jason R.; Gibb, John S.; Genadry, Rene; Burrows, Lara; Lambrou, Nicholas; Buller, Jerome L. (1999)."Anatomy of Pelvic Arteries Adjacent to the Sacrospinous Ligament: Importance of the Coccygeal Branch of the Inferior Gluteal Artery".Obstetrics & Gynecology.94(6). Baltimore, Maryland.: Johns Hopkins University: 973–977.doi:10.1016/s0029-7844(99)00418-4.PMID10576185.
- Platzer, Werner (2004).Color Atlas of Human Anatomy, Vol 1: Locomotor system(5th ed.).Thieme.ISBN3-13-533305-1.(ISBN for the Americas 1-58890-159-9.)
- Vasavada, Sandip P.; Appell, Rodney; Sand, Peter K.; Raz, Shlomo (2004).Female Urology, Urogynecology, and Voiding Dysfunction.Informa Health Care.ISBN0-8247-5426-3.
External links
edit- Anatomy figure: 17:02-03at Human Anatomy Online, SUNY Downstate Medical Center - "Posterior view of the bones and ligaments of the hip joint."
- Johns Hopkins