
Sessile serrated lesion
| Sessile serrated lesion | |
|---|---|
| Other names | Sessile serrated polyp (SSP) Sessile serrated adenoma (SSA) |
 | |
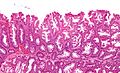
| Micrographof asessile serrated lesion.H&E stain. | |
| Specialty | Gastroenterology |
| Symptoms | Asymptomatic |
| Complications | Colorectal cancer |
| Diagnostic method | Colonoscopy |
| Treatment | Polypectomy |
Asessile serrated lesion(SSL) is apremalignantflat (or sessile) lesion of thecolon,predominantly seen in thececumandascending colon.
SSLs are thought to lead tocolorectal cancerthrough the (alternate)serrated pathway.[1][2]This differs from most colorectal cancer, which arises from mutations starting with inactivation of theAPC gene.
Multiple SSLs may be part of theserrated polyposis syndrome.[3]
Signs and symptoms
[edit]SSLs are generally asymptomatic. They are typically identified on acolonoscopyand excised for a definitive diagnosis and treatment.[citation needed]
Serrated polyposis syndrome
[edit]The serrated polyposis syndrome (SPS) is a relatively rare condition characterized by multiple and/or largeserrated polypsof the colon. Serrated polyps include SSLs, hyperplastic polyps, and traditional serrated adenomas. Diagnosis of this disease is made by the fulfillment of any of the World Health Organization's (WHO) clinical criteria.[4]
Diagnosis
[edit]SSLs are diagnosed by their microscopic appearance;histomorphologically,they are characterized by (1) basal dilation of the crypts, (2) basal crypt serration, (3) crypts that run horizontal to the basement membrane (horizontal crypts), and (4) crypt branching. The most common of these features is basal dilation of the crypts.[citation needed]
Unlike conventional colonicadenomas(e.g. tubular adenoma,villous adenoma), they do not (typically) havenuclearchanges (nuclearhyperchromatism,nuclear crowding, elliptical/cigar-shaped nuclei).[citation needed]
-
 Low magnificationmicrographof an SSL.
Low magnificationmicrographof an SSL. -
 Intermediate magnification micrograph of an SSL.
Intermediate magnification micrograph of an SSL. -
 High magnification micrograph of a SSL showing crypt branching.
High magnification micrograph of a SSL showing crypt branching.



Treatment
[edit]Complete removal of a SSL is considered curative.
Several SSLs confer a higher risk of subsequently findingcolorectal cancerand warrant more frequent surveillance. The surveillance guidelines are the same as for othercolonicadenomas.The surveillance interval is dependent on (1) the number of adenomas, (2) the size of the adenomas, and (3) the presence of high-grade microscopic features.[5]
Epidemiology
[edit]Sessile serrated lesions account for about 25% of all serrated polyps.[6]Advanced SSLs with cytological dysplasia are rare in younger patients,[7]and progression of SSLs appears to be linked with ageing.[8][9]
History
[edit]Sessile serrated adenomas were first described in 1996.[10]In 2019, the World Health Organization recommended the use of the term "sessile serratedlesion,"rather than sessile serratedpolyporadenoma.[6]
See also
[edit]References
[edit]- ^Rüschoff J, Aust D, Hartmann A (2007). "[Colorectal serrated adenoma: diagnostic criteria and clinical implications]".Verh Dtsch Ges Pathol(in German).91:119–25.PMID18314605.
- ^Mäkinen MJ (January 2007). "Colorectal serrated adenocarcinoma".Histopathology.50(1): 131–50.doi:10.1111/j.1365-2559.2006.02548.x.PMID17204027.S2CID2377929.
- ^Rosty, C.; Parry, S.; Young, JP. (2011)."Serrated polyposis: an enigmatic model of colorectal cancer predisposition".Pathol Res Int.2011:157073.doi:10.4061/2011/157073.PMC3109311.PMID21660283.
- ^World J Gastroenterol 2012 May 28; 18(20): 2452–2461
- ^Levine JS, Ahnen DJ (December 2006). "Clinical practice. Adenomatous polyps of the colon".N. Engl. J. Med.355(24): 2551–7.doi:10.1056/NEJMcp063038.PMID17167138.
- ^abCrockett, SD; Nagtegaal, ID (October 2019)."Terminology, Molecular Features, Epidemiology, and Management of Serrated Colorectal Neoplasia".Gastroenterology.157(4): 949–966.e4.doi:10.1053/j.gastro.2019.06.041.PMID31323292.
- ^Bettington, Mark; Walker, Neal; Rosty, Christophe; Brown, Ian; Clouston, Andrew; McKeone, Diane; Pearson, Sally-Ann; Leggett, Barbara; Whitehall, Vicki (January 2017). "Clinicopathological and molecular features of sessile serrated adenomas with dysplasia or carcinoma".Gut.66(1): 97–106.doi:10.1136/gutjnl-2015-310456.PMID26475632.S2CID3495692.
- ^Fennell, Lochlan; Kane, Alexandra; Liu, Cheng; McKeone, Diane; Hartel, Gunter; Su, Chang; Bond, Catherine; Bettington, Mark; Leggett, Barbara; Whitehall, Vicki (6 July 2021)."Braf mutation induces rapid neoplastic transformation in the aged and aberrantly methylated intestinal epithelium".Gut.71(6): gutjnl–2020–322166.doi:10.1136/gutjnl-2020-322166.PMC9120393.PMID34230216.
- ^Bettington, M; Brown, I; Rosty, C; Walker, N; Liu, C; Croese, J; Rahman, T; Pearson, SA; McKeone, D; Leggett, B; Whitehall, V (March 2019). "Sessile Serrated Adenomas in Young Patients may have Limited Risk of Malignant Progression".Journal of Clinical Gastroenterology.53(3): e113–e116.doi:10.1097/MCG.0000000000001014.PMID29570172.S2CID4261352.
- ^Torlakovic, E; Snover, DC (July 2006). "Sessile serrated adenoma: a brief history and current status".Critical Reviews in Oncogenesis.12(1–2): 27–39.doi:10.1615/critrevoncog.v12.i1-2.30.PMID17078205.